

Pre-existing mutations related to tenofovir in chronic hepatitis B patients with long-term nucleos(t)ide analogue drugs treatment by ultra-deep pyrosequencing
- PMID: 27602500
- PMCID: PMC5342551
- DOI: 10.18632/oncotarget.11840
Pre-existing mutations related to tenofovir in chronic hepatitis B patients with long-term nucleos(t)ide analogue drugs treatment by ultra-deep pyrosequencing
Abstract
Aims: The dynamics of resistance-associated mutations under combination therapy were explored.
Methods: A total of 46 patients were classified into adefovir (n=14) and entecavir (n=32) groups. In the adefovir (ADV) group, six patients receiving combined therapy were DNA-positive after more than 3 years of therapy. Ultra-deep pyrosequencing was used to analyze the dynamics of multi-drugs resistance mutations.
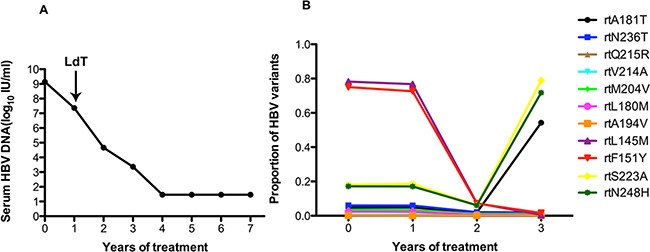
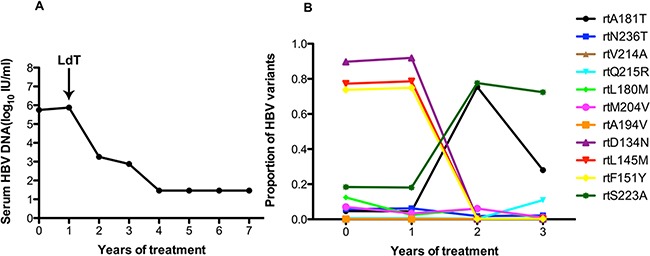
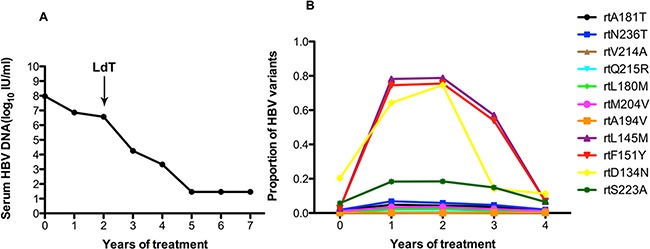
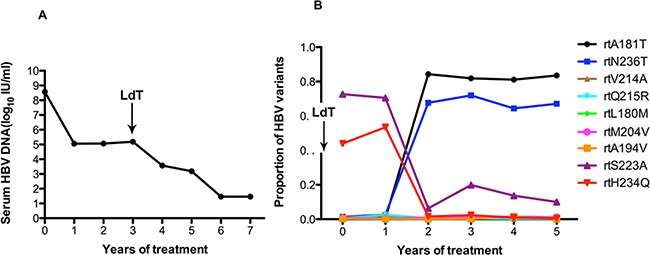
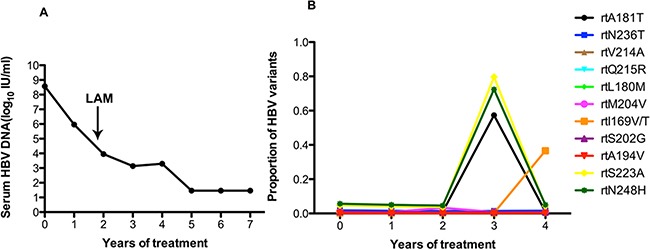
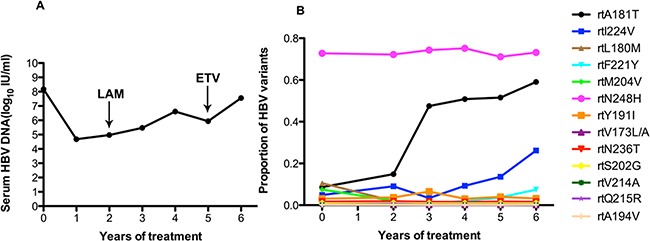
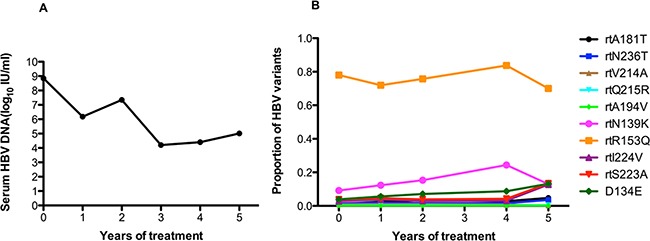
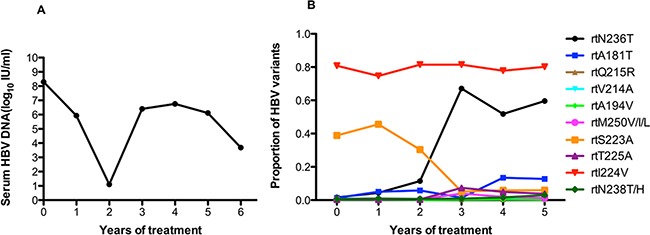
Results: At baseline, all 46 treatment-naïve patients harbored rtA181V/T substitutions (1.2%-4.6%) and rtN236T substitutions (1.6%-6.1%). In the ADV group, eight patients with long-term treatment were consecutively HBV DNA-positive for more than 3 years. During treatment, the rtA181T resistance-associated site appeared with increasing frequency in six of eight patients (NOs. 1-6), and two patients (NOs.4 and 8) carrying the rtA181T resistance mutations increasingly showed high levels of rtN236T. One patient (NO. 8) experienced virological breakthrough. Other known pre-existing mutations showed no dynamic fluctuations, including in rtA194T, rtP177G, rtF249A, and rtD263E. In addition to the common substitutions, some previously unknown amino acid substitutions, such as rtD134N, rtL145M/S, rtF151Y/L, rtR153Q, and rtS223A, should be further studied.
Conclusions: HBV-resistance substitutions conferring to nucleoside analogs are present at baseline. The dynamics of the HBV RT-region quasispecies variation are heterogeneous and complex.
Keywords: hepatitis B virus; multi-drugs therapy; resistance; tenofovir; ultra-deep pyrosequencing.
Conflict of interest statement
All authors declare that they have no competing interests.
Figures
Similar articles
-
Tenofovir rescue regimen following prior suboptimal response to entecavir and adefovir combination therapy in chronic hepatitis B patients exposed to multiple treatment failures.J Med Virol. 2015 Jun;87(6):1013-21. doi: 10.1002/jmv.24153. Epub 2015 Feb 25. J Med Virol. 2015. PMID: 25716029
-
Viral evolutionary changes during tenofovir treatment in a chronic hepatitis B patient with sequential nucleos(t)ide therapy.J Clin Virol. 2014 Jul;60(3):313-6. doi: 10.1016/j.jcv.2014.03.018. Epub 2014 Apr 12. J Clin Virol. 2014. PMID: 24836314
-
Tenofovir has inferior efficacy in adefovir-experienced chronic hepatitis B patients compared to nucleos(t)ide-naïve patients.Clin Mol Hepatol. 2017 Mar;23(1):66-73. doi: 10.3350/cmh.2016.0060. Epub 2017 Feb 14. Clin Mol Hepatol. 2017. PMID: 28190329 Free PMC article.
-
In vitro susceptibility of adefovir-associated hepatitis B virus polymerase mutations to other antiviral agents.Antivir Ther. 2007;12(3):355-62. Antivir Ther. 2007. PMID: 17591025
-
[Resistance to adefovir in patients with chronic hepatitis B].Korean J Hepatol. 2006 Dec;12(4):484-92. Korean J Hepatol. 2006. PMID: 17237626 Review. Korean.
Cited by
-
Understanding the genetics of viral drug resistance by integrating clinical data and mining of the scientific literature.Sci Rep. 2022 Aug 25;12(1):14476. doi: 10.1038/s41598-022-17746-3. Sci Rep. 2022. PMID: 36008431 Free PMC article.
-
Naturally occurring hepatitis B virus reverse transcriptase mutations related to potential antiviral drug resistance and liver disease progression.World J Gastroenterol. 2018 Apr 28;24(16):1708-1724. doi: 10.3748/wjg.v24.i16.1708. World J Gastroenterol. 2018. PMID: 29713126 Free PMC article. Review.
-
Prevalence of Potential Resistance Related Variants Among Chinese Chronic Hepatitis B Patients Not Receiving Nucleos(T)ide Analogues.Infect Drug Resist. 2020 Jul 17;13:2407-2416. doi: 10.2147/IDR.S249476. eCollection 2020. Infect Drug Resist. 2020. PMID: 32765014 Free PMC article.
References
-
- Fung S, Kwan P, Fabri M, Horban A, Pelemis M, Hann HW, Gurel S, Caruntu FA, Flaherty JF, Massetto B, Dinh P, Corsa A, Subramanian GM, et al. Randomized comparison of tenofovir disoproxil fumarate vs emtricitabine and tenofovir disoproxil fumarate in patients with lamivudine-resistant chronic hepatitis B. Gastroenterology. 2014;146:980–988. doi: 10.1053/j.gastro.2013.12.028. - DOI - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
