

Biopsy-free circulating tumor DNA assay identifies actionable mutations in lung cancer
- PMID: 27602770
- PMCID: PMC5341844
- DOI: 10.18632/oncotarget.11801
Biopsy-free circulating tumor DNA assay identifies actionable mutations in lung cancer
Abstract
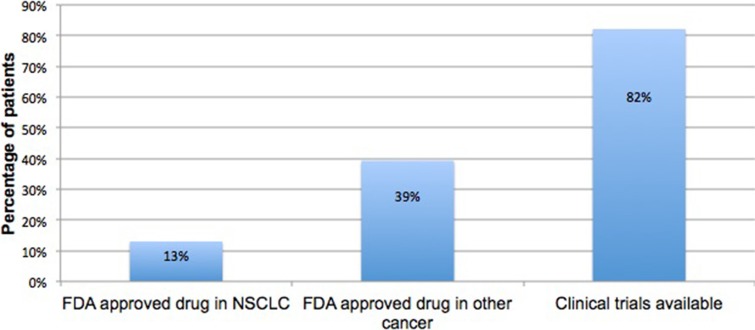
Introduction: The potential of oncogene-driven targeted therapy is perhaps most fully realized in non-small cell lung cancer (NSCLC), given the number of genomic targets and approved matched therapies. However, invasive tissue biopsy at the time of each disease progression may not be possible and is associated with high morbidity and cost. Use of newly available "liquid biopsies" can circumvent these issues.
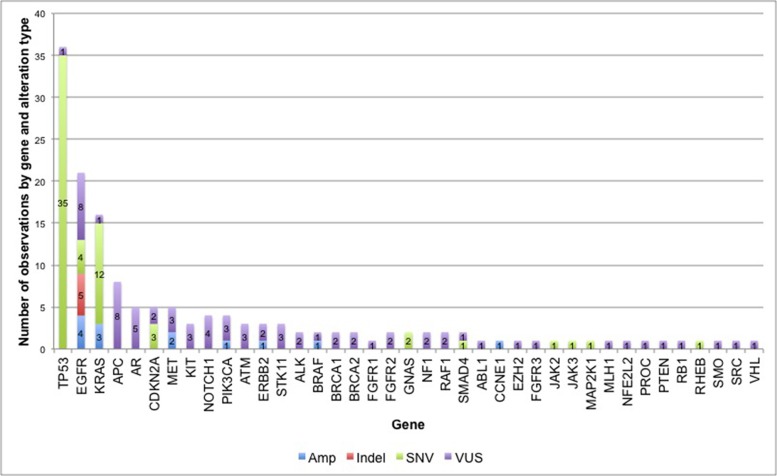
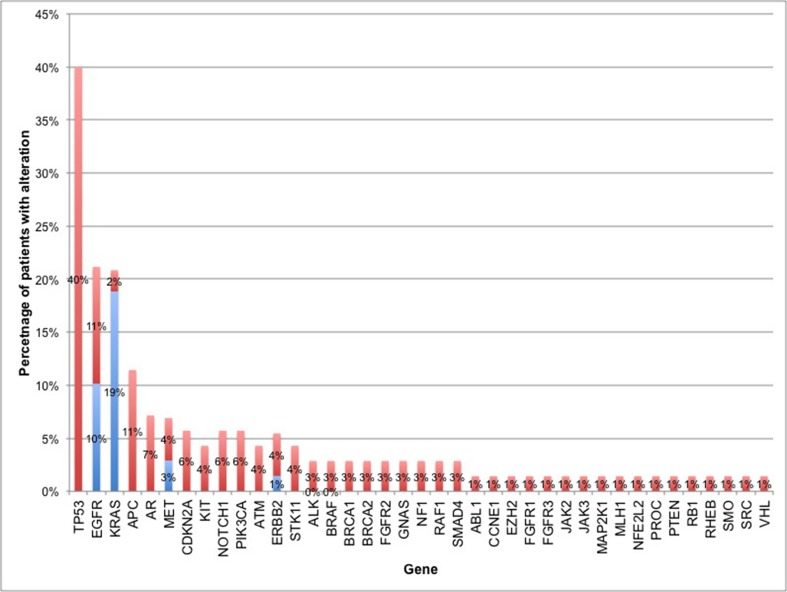
Results: 83% of subjects had at least one genomic alteration identified in plasma. Most commonly mutated genes were TP53, KRAS and EGFR. Subjects with no detectable ctDNA were more likely to have small volume disease, lepidic growth pattern, mucinous tumors or isolated leptomeningeal disease.
Methods: Subjects were individuals with NSCLC undergoing analysis of cell-free circulating tumor DNA using a validated, commercially-available next-generation sequencing assay at a single institution. Demographic, clinicopathologic information and results from tissue and plasma-based genomic testing were reviewed for each subject.
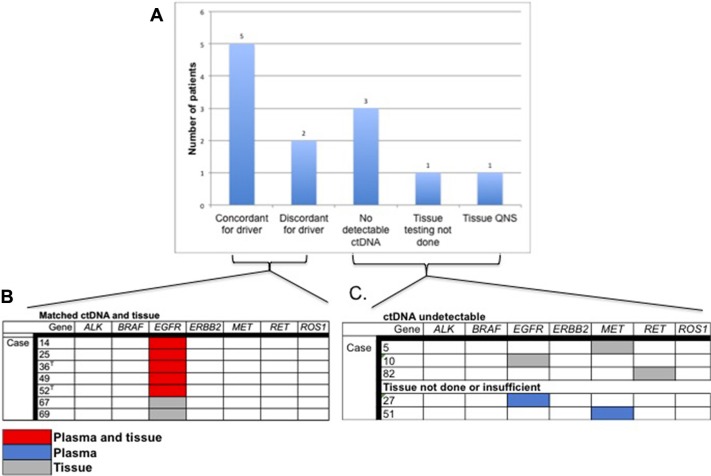
Conclusions: This is the first clinic-based series of NSCLC patients assessing outcomes of targeted therapies using a commercially available ctDNA assay. Over 80% of patients had detectable ctDNA, concordance between paired tissue and blood for truncal oncogenic drivers was high and patients with biomarkers identified in plasma had PFS in the expected range. These data suggest that biopsy-free ctDNA analysis is a viable first choice when the diagnostic tissue biopsy is insufficient for genotyping or at the time of progression when a repeated invasive tissue biopsy is not possible/preferred.
Keywords: cell-free DNA; circulating tumor DNA; next-generation sequencing; non-small cell lung cancer.
Conflict of interest statement
Conflicts of Interest and Source of Funding: BN, KB, RBL and AT are employees of and hold equity in Guardant Health, Inc.
Figures
References
-
- Mok TS, Wu YL, Thongprasert S, Yang CH, Chu DT, Saijo N, Sunpaweravong P, Han B, Margono B, Ichinose Y, Nishiwaki Y, Ohe Y, Yang JJ, et al. Gefitinib or carboplatin-paclitaxel in pulmonary adenocarcinoma. N Engl J Med. 2009;361:947–957. - PubMed
-
- Zhou C, Wu YL, Chen G, Feng J, Liu XQ, Wang C, Zhang S, Wang J, Zhou S, Ren S, Lu S, Zhang L, Hu C, et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011;12:735–742. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
Research Materials
Miscellaneous
