

Review
doi: 10.1259/bjr.20160347.
Epub 2016 Sep 26.
Cardiothoracic manifestations of primary histiocytoses
Affiliations
- PMID: 27603510
- PMCID: PMC5604911
- DOI: 10.1259/bjr.20160347
Item in Clipboard
Review
Cardiothoracic manifestations of primary histiocytoses
Br J Radiol.
2016 Dec.
Abstract
The objectives of this article were: (1) to review common and rare manifestations of systemic and pulmonary Langerhans cell histiocytosis, Rosai-Dorfman disease, Erdheim-Chester disease and juvenile xanthogranuloma; (2) to provide the reader with important pathologic, epidemiologic and clinical features of these diseases. The histiocytoses are a diverse group of diseases which typically manifest with multiorgan involvement. Understanding the pathologic, epidemiologic and clinical features of these entities can help the radiologist suggest an accurate diagnosis of histiocytosis when typical imaging features are encountered.
Figures

Systemic Langerhans cell histiocytosis (LCH) in an infant: chest radiograph (a) in an infant with systemic LCH is showing diffuse reticular opacities. Accompanying CT (b) is demonstrating extensive cysts and areas of architectural distortion.

Mediastinal and vertebral involvement in systemic Langerhans cell histiocytosis (LCH): contrast-enhanced chest CT (a) in an infant with systemic LCH is showing extensive coalescent lymphadenopathy throughout the mediastinum resulting in compression and displacement of vascular and other mediastinal structures. Sagittal T2 weighted MR image of the cervicothoracic spine (b) in a 6-year-old female is showing diffuse, severe loss of height of the T1 vertebral body (arrow) with mild retropulsion into the spinal canal. These findings are compatible with the vertebra plana and have been pathologically proven to represent LCH involvement.

Adolescent male with systemic LCH. Coronal fused FDG PET-CT (a) and coronal CT (b) images demonstrating scattered upper lobe predominant FDG-avid irregular, slightly spiculated nodules with cavitation and cyst formation.

Pulmonary Langerhans cell histiocytosis (pLCH) in multiple patients: CT of the chest (a) in a 48-year-old female smoker is demonstrating upper lobe predominant bizarre cysts and scattered nodules (arrows). Coronal CT of the chest (b) in a different patient is showing more severe disease with replacement of parenchyma by multiple upper lobe predominant coalescent cysts, mimicking emphysema. It can be noted that the disease has spared the costophrenic angles. CT of the chest in a 44-year-old female (c) is showing a loculated pneumothorax complicating pLCH (star).

Airways and lung involvement in Rosai-Dorfman disease. Coronal contrast enhanced CT image (a) through the laryngeal region demonstrating mass-like thickening of the right subglottic mucosa (arrow). Axial contrast enhanced CT image through the upper trachea (b) shows subtle mass-like thickening of the right lateral tracheal wall (arrow). Axial CT image through the upper lobes (c) shows a spiculated right upper lobe nodule (arrow).

Mediastinal involvement in Rosai–Dorfman disease (RDD): axial CT images in two different patients with RDD at the level of the aortopulmonary window (a) and left main pulmonary artery (b) are showing coalescent lymphadenopathy and infiltrative soft tissue in the mediastinum (stars in a and b).
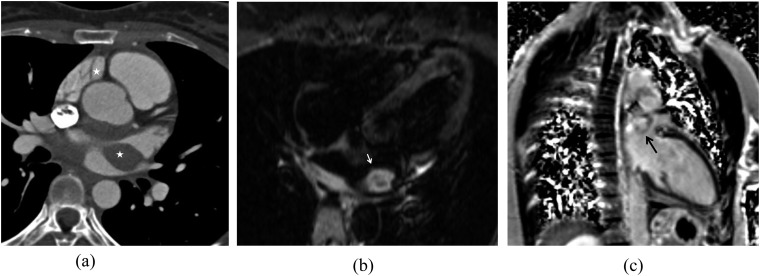
A cardiac mass in a patient with Rosai–Dorfman disease: contrast-enhanced electrocardiogram-gated CT of the heart (a) is demonstrating a soft-tissue density mass centred about the left atrium (stars). T2 weighted four-chamber MR image (b) of the heart is showing a T2 hyperintense left atrial mass (white arrow). After the injection of contrast on the phase-sensitive inversion-recovery sequence (c), this mass is demonstrating delayed enhancement (black arrow).

Interstitial lung disease in two patients with Erdheim–Chester disease (ECD): CT images of the chest in a 74-year-old female (a) with ECD in the lung window is demonstrating smooth interlobular septal thickening and scattered areas of ground-glass opacity. Contrast CT of the chest in lung window in a 54-year-old male (b) is depicting more severe pulmonary involvement characterized by interlobular septal thickening, ill-defined ground-glass nodules, intralobular lines, ground-glass opacity and scattered bronchiectasis. Extensive pleural thickening can also be noted.

Cardiomediastinal involvement in three patients with Erdheim–Chester disease: non-contrast CT of the chest through the heart (a) is showing epicardial and posterior mediastinal infiltrative soft tissue (arrows). Fused positron emission tomography-CT image in a different patient (b) is demonstrating a highly hypermetabolic infiltrative soft tissue in an epicardial distribution about the right atrium (arrows). The patient additionally has a small right pleural effusion as well as a fludeoxyglucose-avid right lower lobe histopathologically confirmed primary lung neoplasm (arrowhead). CT of the chest at the level of the heart in another patient (c) is demonstrating extensive soft tissue infiltrating the epicardium. This soft tissue is encasing the right coronary artery (arrow) in the right atrioventricular groove. There is extensive posterior mediastinal soft tissue that has displaced the descending aorta anteriorly. In addition, significant left pleural thickening is present.

Juvenile xanthogranuloma in a 3-month-old infant: coronal (a) and axial (b) T2 weighted MR images of the chest are demonstrating multiple T2 hyperintese nodules throughout the lung parenchyma as well as in the liver.
References
-
- Favara BE, Feller AC, Pauli M, Jaffe ES, Weiss LM, Arico M, et al. . Contemporary classification of histiocytic disorders. The WHO committee on histiocytic/reticulum cell proliferations. Reclassification working group of the histiocyte society. Med Pediatr Oncol 1997; 29: 157–66. doi: https://doi.org/10.1002/(SICI)1096-911X(199709)29:3<157::AID-MPO1>3.0.CO... - DOI - PubMed
-
- Jaffe R. The histiocytoses. Clin Lab Med 1999; 19: 135–55. - PubMed
-
- Katz SI, Tamaki K, Sachs DH. Epidermal langerhans cells are derived from cells originating in bone marrow. Nature 1979; 282: 324–6. doi: https://doi.org/10.1038/282324a0 - DOI - PubMed
-
- Lieberman PH, Jones CR, Steinman RM, Erlandson RA, Smith J, Gee T, et al. . Langerhans cell (eosinophilic) granulomatosis. A clinicopathologic study encompassing 50 years. Am J Surg Pathol 1996; 20: 519–52. doi: https://doi.org/10.1097/00000478-199605000-00001 - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
