

Complement 5a is an indicator of significant fibrosis and earlier cirrhosis in patients chronically infected with hepatitis B virus
- PMID: 27605044
- PMCID: PMC5306372
- DOI: 10.1007/s15010-016-0942-7
Complement 5a is an indicator of significant fibrosis and earlier cirrhosis in patients chronically infected with hepatitis B virus
Abstract
Purpose: To investigate the association between serum complement 5a (C5a) concentration and liver fibrosis and cirrhosis in a large cohort of patients chronically infected with hepatitis B virus (HBV).
Methods: Five hundred and eight patients with chronic HBV infection undergoing liver biopsy were included. Serum concentrations of C5a was measured by Luminex screening system. Ishak histological system was obtained.
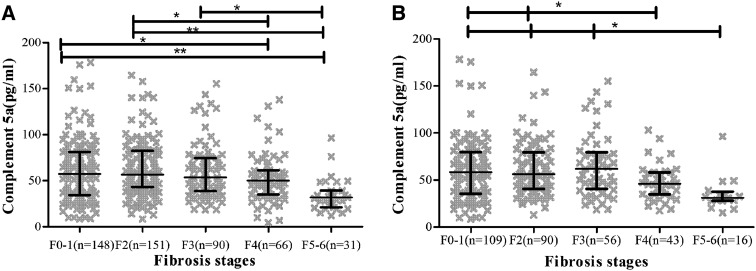
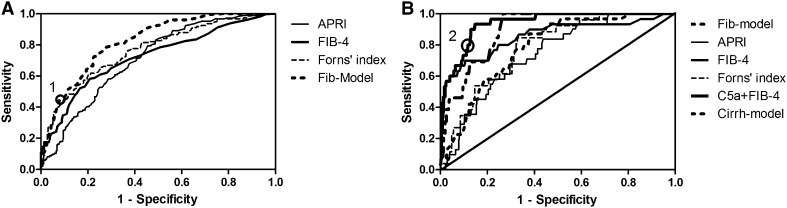
Results: C5a levels were negatively associated with liver fibrosis stages and significantly declined in patients with severe fibrosis and cirrhosis (P < 0.001). Multiple analysis showed C5a, AST, laminin, Co-IV, platelet count, albumin, HBsAg associated with liver fibrosis independently. Based on the markers above, we created two scores, Fib-model for significant fibrosis and Cirrh-model for earlier cirrhosis. Fib-model was performing better to differentiate from significant fibrosis, with an AUROC of 0.82 (95 % CI 0.78, 0.86), in comparison to existed models APRI, FIB-4 and Forns' index with AUROCs of 0.71 (95 % CI 0.66, 0.76), 0.72 (95 % CI 0.67, 0.77), 0.77 (95 % CI 0.72, 0.81), respectively. Although, Cirrh-model showed AUROC of 0.85 (95 % CI 0.80, 0.91) for evaluation of earlier cirrhosis, superior to APRI, and Forns' index, C5a + FIB-4 performed best with an AUROC of 0.94 (95 % CI 0.90, 0.97).
Conclusion: In patients with chronic HBV infection, serum C5a concentration significantly decreased in severe fibrosis stages and earlier cirrhosis. Fib-model and C5a + FIB-4 performed better than existed models for assessment of significant fibrosis and earlier cirrhosis, respectively.
Keywords: Cirrhosis; Complement 5a; Hepatitis B; Liver fibrosis.
Conflict of interest statement
Compliance with ethical standardsConflict of interestNone.FundingThis study was supported by China Mega-Project for Infectious Diseases (Grant Numbers 2013ZX10002005, 2012ZX10002006, 2013ZX10002004, 2012ZX10005005), Project of Beijing Science and Technology Committee (Grant Number D121100003912002).
Figures
Similar articles
-
The gamma-glutamyl transpeptidase-to-platelet ratio predicts liver fibrosis and cirrhosis in HBeAg-positive chronic HBV infection patients with high HBV DNA and normal or mildly elevated alanine transaminase levels in China.J Viral Hepat. 2016 Nov;23(11):912-919. doi: 10.1111/jvh.12563. Epub 2016 Jul 4. J Viral Hepat. 2016. PMID: 27375134
-
The gamma-glutamyl transpeptidase to platelet ratio for non-invasive assessment of liver fibrosis in patients with chronic hepatitis B and non-alcoholic fatty liver disease.Oncotarget. 2017 Apr 25;8(17):28641-28649. doi: 10.18632/oncotarget.16162. Oncotarget. 2017. PMID: 28415736 Free PMC article.
-
The Gamma-Glutamyl-Transpeptidase to Platelet Ratio Does not Show Advantages than APRI and Fib-4 in Diagnosing Significant Fibrosis and Cirrhosis in Patients With Chronic Hepatitis B: A Retrospective Cohort Study in China.Medicine (Baltimore). 2016 Apr;95(16):e3372. doi: 10.1097/MD.0000000000003372. Medicine (Baltimore). 2016. PMID: 27100421 Free PMC article.
-
Serum HBV RNA levels predict significant liver fibrosis in patients with chronic HBV infection.Discov Med. 2020 Mar-Apr;29(157):119-128. Discov Med. 2020. PMID: 33002408
-
Quantification of liver fibrosis in chronic hepatitis B virus infection.J Med Life. 2015 Jul-Sep;8(3):285-90. J Med Life. 2015. PMID: 26351528 Free PMC article. Review.
Cited by
-
Complement 5a Receptor deficiency does not influence adverse cardiac remodeling after pressure-overload in mice.Sci Rep. 2017 Dec 6;7(1):17045. doi: 10.1038/s41598-017-16957-3. Sci Rep. 2017. PMID: 29213128 Free PMC article.
-
Serum angiotensin-converting enzyme level for evaluating significant fibrosis in chronic hepatitis B.World J Gastroenterol. 2017 Sep 28;23(36):6705-6714. doi: 10.3748/wjg.v23.i36.6705. World J Gastroenterol. 2017. PMID: 29085215 Free PMC article.
-
Complement System and Adhesion Molecule Skirmishes in Fabry Disease: Insights into Pathogenesis and Disease Mechanisms.Int J Mol Sci. 2024 Nov 14;25(22):12252. doi: 10.3390/ijms252212252. Int J Mol Sci. 2024. PMID: 39596318 Free PMC article. Review.
-
Research progress on the roles of complement in liver injury.World J Hepatol. 2025 Mar 27;17(3):103839. doi: 10.4254/wjh.v17.i3.103839. World J Hepatol. 2025. PMID: 40177195 Free PMC article. Review.
-
The complement system in liver diseases: Evidence-based approach and therapeutic options.J Transl Autoimmun. 2019 Sep 18;2:100017. doi: 10.1016/j.jtauto.2019.100017. eCollection 2019 Dec. J Transl Autoimmun. 2019. PMID: 32743505 Free PMC article. Review.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
