

Non-invasive Model-Based Assessment of Passive Left-Ventricular Myocardial Stiffness in Healthy Subjects and in Patients with Non-ischemic Dilated Cardiomyopathy
- PMID: 27605213
- PMCID: PMC5479360
- DOI: 10.1007/s10439-016-1721-4
Non-invasive Model-Based Assessment of Passive Left-Ventricular Myocardial Stiffness in Healthy Subjects and in Patients with Non-ischemic Dilated Cardiomyopathy
Abstract
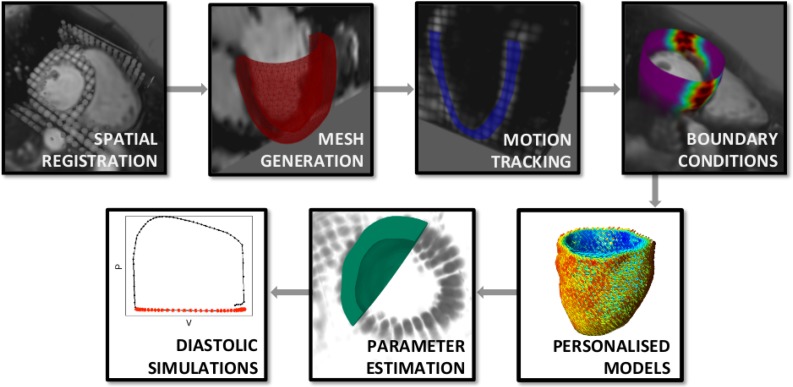
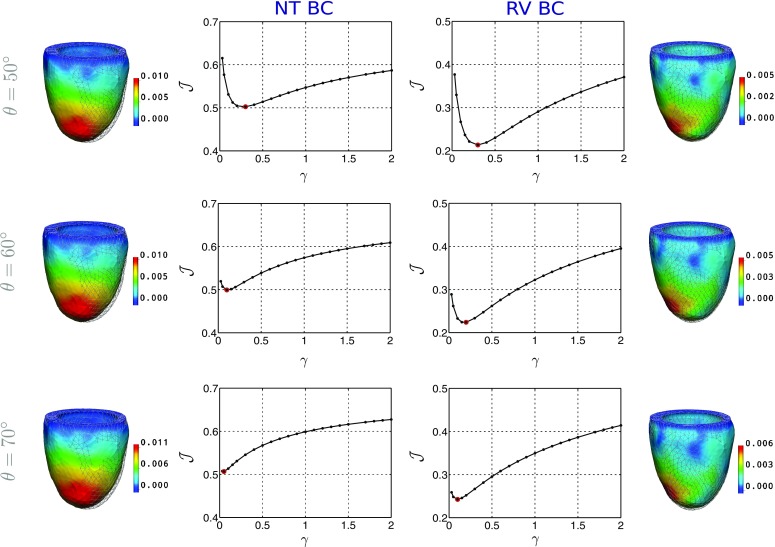
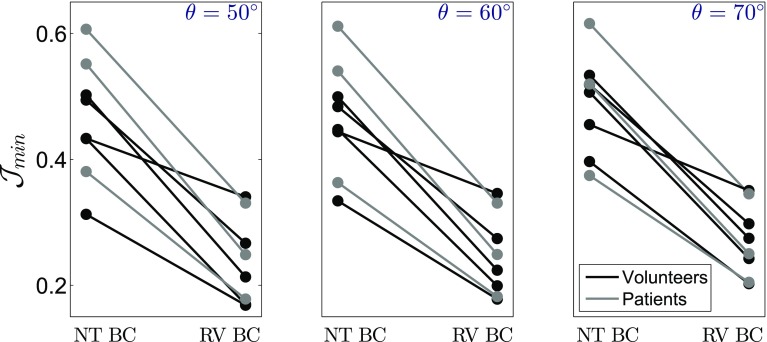
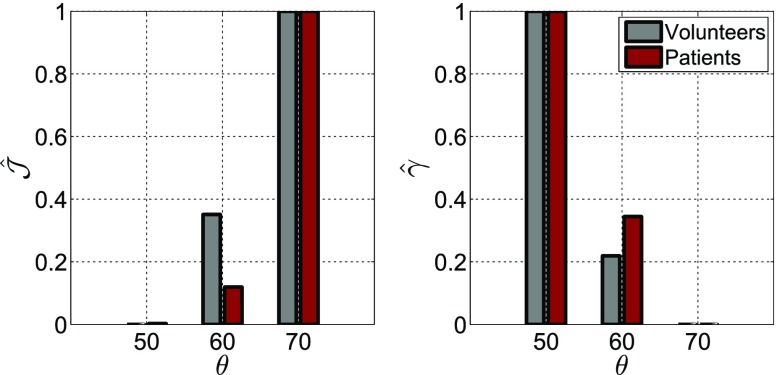
Patient-specific modelling has emerged as a tool for studying heart function, demonstrating the potential to provide non-invasive estimates of tissue passive stiffness. However, reliable use of model-derived stiffness requires sufficient model accuracy and unique estimation of model parameters. In this paper we present personalised models of cardiac mechanics, focusing on improving model accuracy, while ensuring unique parametrisation. The influence of principal model uncertainties on accuracy and parameter identifiability was systematically assessed in a group of patients with dilated cardiomyopathy ([Formula: see text]) and healthy volunteers ([Formula: see text]). For all cases, we examined three circumferentially symmetric fibre distributions and two epicardial boundary conditions. Our results demonstrated the ability of data-derived boundary conditions to improve model accuracy and highlighted the influence of the assumed fibre distribution on both model fidelity and stiffness estimates. The model personalisation pipeline-based strictly on non-invasive data-produced unique parameter estimates and satisfactory model errors for all cases, supporting the selected model assumptions. The thorough analysis performed enabled the comparison of passive parameters between volunteers and dilated cardiomyopathy patients, illustrating elevated stiffness in diseased hearts.
Keywords: Model uncertainties; Myocardium; Parameter uniqueness; Patient-specific modelling; Stiffness.
Figures
Similar articles
-
Characterizing variability in passive myocardial stiffness in healthy human left ventricles using personalized MRI and finite element modeling.Sci Rep. 2025 Feb 14;15(1):5556. doi: 10.1038/s41598-025-89243-2. Sci Rep. 2025. PMID: 39953070 Free PMC article.
-
Improved identifiability of myocardial material parameters by an energy-based cost function.Biomech Model Mechanobiol. 2017 Jun;16(3):971-988. doi: 10.1007/s10237-016-0865-3. Epub 2017 Feb 10. Biomech Model Mechanobiol. 2017. PMID: 28188386 Free PMC article.
-
Functional and structural abnormalities in patients with dilated cardiomyopathy.J Am Coll Cardiol. 1989 Sep;14(3):613-23. doi: 10.1016/0735-1097(89)90102-2. J Am Coll Cardiol. 1989. PMID: 2768711
-
Personalized evaluation of the passive myocardium in ischemic cardiomyopathy via computational modeling using Bayesian optimization.Biomech Model Mechanobiol. 2024 Oct;23(5):1591-1606. doi: 10.1007/s10237-024-01856-0. Epub 2024 Jul 2. Biomech Model Mechanobiol. 2024. PMID: 38954283
-
Myocardial segmental thickness variability on echocardiography is a highly sensitive and specific marker to distinguish ischemic and non-ischemic dilated cardiomyopathy in new onset heart failure.Int J Cardiovasc Imaging. 2019 May;35(5):791-798. doi: 10.1007/s10554-018-01515-3. Epub 2018 Dec 29. Int J Cardiovasc Imaging. 2019. PMID: 30594979 Free PMC article.
Cited by
-
Efficient Ventricular Parameter Estimation Using AI-Surrogate Models.Front Physiol. 2021 Oct 14;12:732351. doi: 10.3389/fphys.2021.732351. eCollection 2021. Front Physiol. 2021. PMID: 34721062 Free PMC article.
-
An efficient and accurate method for modeling nonlinear fractional viscoelastic biomaterials.Comput Methods Appl Mech Eng. 2020 Apr 15;362:112834. doi: 10.1016/j.cma.2020.112834. eCollection 2020 Apr 15. Comput Methods Appl Mech Eng. 2020. PMID: 34136022 Free PMC article.
-
Dobutamine stress testing in patients with Fontan circulation augmented by biomechanical modeling.PLoS One. 2020 Feb 21;15(2):e0229015. doi: 10.1371/journal.pone.0229015. eCollection 2020. PLoS One. 2020. PMID: 32084180 Free PMC article.
-
Monitoring of cardiovascular physiology augmented by a patient-specific biomechanical model during general anesthesia. A proof of concept study.PLoS One. 2020 May 14;15(5):e0232830. doi: 10.1371/journal.pone.0232830. eCollection 2020. PLoS One. 2020. PMID: 32407353 Free PMC article.
-
Physical model of end-diastolic and end-systolic pressure-volume relationships of a heart.Front Physiol. 2023 Aug 21;14:1195502. doi: 10.3389/fphys.2023.1195502. eCollection 2023. Front Physiol. 2023. PMID: 37670768 Free PMC article.
References
-
- Alter P, Rupp H, Rominger M, Klose K, Maisch B. A new methodological approach to assess cardiac work by pressure-volume and stress-length relations in patients with aortic valve stenosis and dilated cardiomyopathy. Pflüg. Arch. Eur. J. Phys. 2008;455:627–636. doi: 10.1007/s00424-007-0323-2. - DOI - PubMed
-
- Asner, L., Hadjicharalambous, M., Chabiniok, R., Peresutti, D., Sammut, E., Wong, J., Carr-White, G., Chowienczyk, P., Lee, J., King, A., Smith, N., Razavi, R., and Nordsletten D. Estimation of passive and active properties in the human heart using 3D tagged MRI. Biomech. Model. Mechanobiol. 2015. doi:10.1007/s10237-015-0748-z. - PMC - PubMed
-
- Asner LM, Hadjicharalambous M, Lee J, Nordsletten D. Stacom challenge: simulating left ventricular mechanics in the canine heart. In: Camara O, Mansi T, Pop M, Rhode K, Sermesant M, Young A, editors. Statistical Atlases and Computational Models of the Heart—Imaging and Modelling Challenges. New York: Springer; 2015. pp. 123–134.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
