

The Survival Benefit of "Fistula First, Catheter Last" in Hemodialysis Is Primarily Due to Patient Factors
- PMID: 27605542
- PMCID: PMC5280011
- DOI: 10.1681/ASN.2016010019
The Survival Benefit of "Fistula First, Catheter Last" in Hemodialysis Is Primarily Due to Patient Factors
Abstract
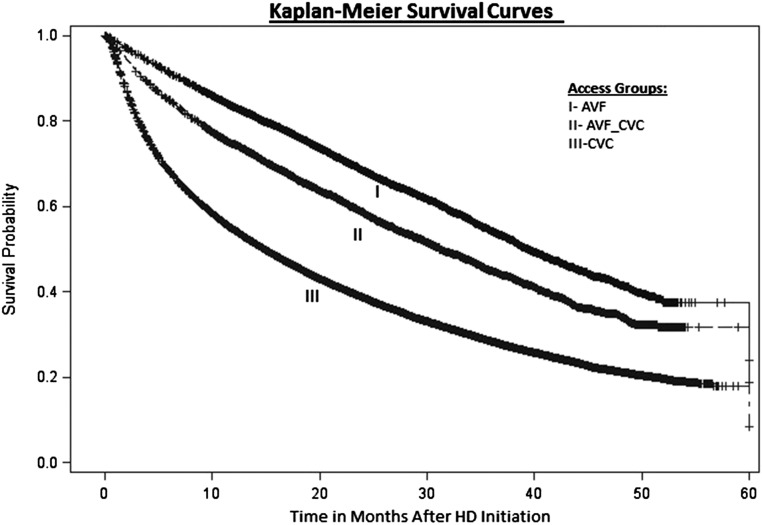
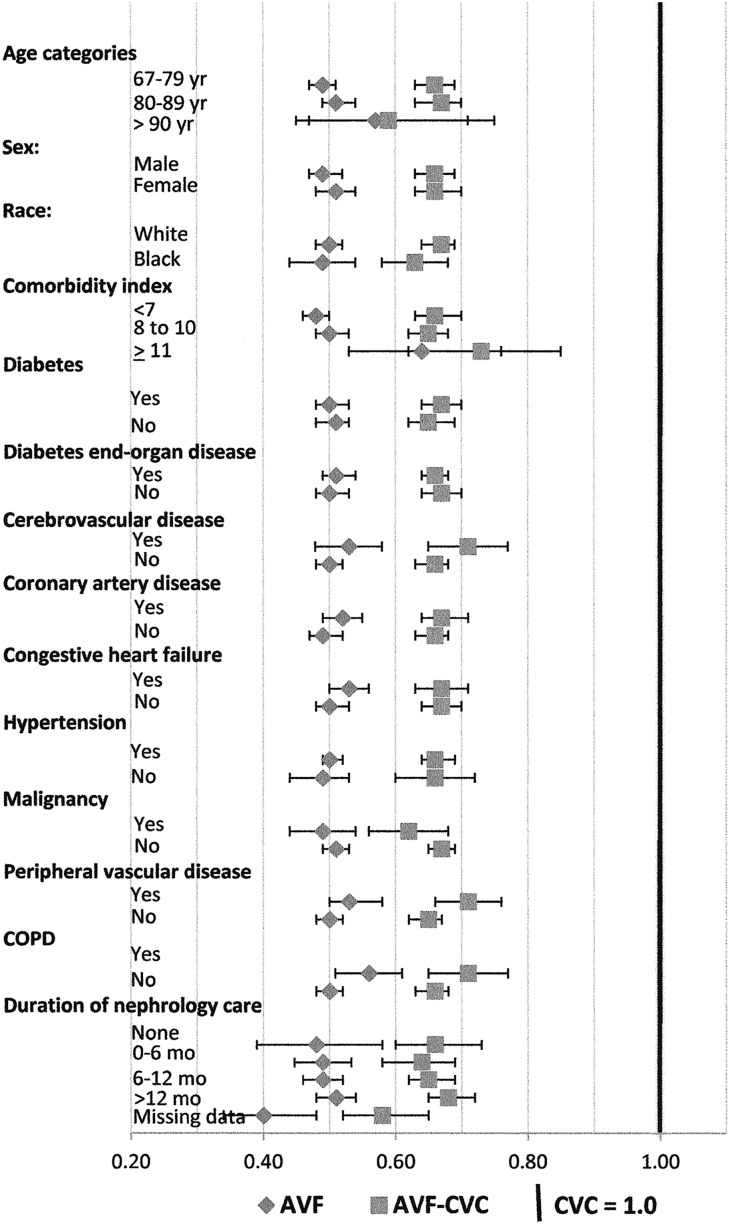
Patients needing hemodialysis are advised to have arteriovenous fistulas rather than catheters because of significantly lower mortality rates. However, disparities in fistula placement raise the possibility that patient factors have a role in this apparent mortality benefit. We derived a cohort of 115,425 patients on incident hemodialysis ≥67 years old from the US Renal Data System with linked Medicare claims to identify the first predialysis vascular access placed. We compared mortality outcomes in patients initiating hemodialysis with a fistula placed first, a catheter after a fistula placed first failed, or a catheter placed first (n=90,517; reference group). Of 21,436 patients with a fistula placed first, 9794 initiated hemodialysis with that fistula, and 8230 initiated dialysis with a catheter after failed fistula placement. The fistula group had the lowest mortality over 58 months (hazard ratio, 0.50; 95% confidence interval, 0.48 to 0.52; P<0.001), with mortality rates at 6, 12, and 24 months after initiation of 9%, 17%, and 31%, respectively, compared with 32%, 46%, and 62%, respectively, in the catheter group. However, the group initiating hemodialysis with a catheter after failed fistula placement also had significantly lower mortality rates than the catheter group had over 58 months (hazard ratio, 0.66; 95% confidence interval, 0.64 to 0.68; P<0.001), with mortality rates of 15%, 25%, and 42% at 6, 12, and 24 months, respectively. Thus, patient factors affecting fistula placement, even when patients are hemodialyzed with a catheter instead, may explain at least two thirds of the mortality benefit observed in patients with a fistula.
Keywords: access; arteriovenous fistula; dialysis; hemodialysis access; mortality; mortality risk.
Copyright © 2017 by the American Society of Nephrology.
Figures
Comment in
-
Vascular Access for Hemodialysis and Value-Based Purchasing for ESRD.J Am Soc Nephrol. 2017 Feb;28(2):395-397. doi: 10.1681/ASN.2016070769. Epub 2016 Oct 6. J Am Soc Nephrol. 2017. PMID: 28143965 Free PMC article. No abstract available.
References
-
- NKF-K/DOQI : III. NKF-K/DOQI clinical practice guidelines for vascular access: Update 2000. Am J Kidney Dis 37[Suppl 1]: S137–S181, 2001 - PubMed
-
- Lok CE: Fistula first initiative: Advantages and pitfalls. Clin J Am Soc Nephrol 2: 1043–1053, 2007 - PubMed
-
- Allon M: Current management of vascular access. Clin J Am Soc Nephrol 2: 786–800, 2007 - PubMed
-
- Lacson E Jr., Lazarus JM, Himmelfarb J, Ikizler TA, Hakim RM: Balancing fistula first with catheters last. Am J Kidney Dis 50: 379–395, 2007 - PubMed
-
- End Stage Renal Disease (ESRD) National Coordinating Center (NCC): Fistula First Catheter Last—FFCL. Available at: http://esrdncc.org/ffcl/. Accessed January 4, 2016
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
