

Distinguishing Arterial Ischemic Stroke From Hypoxic-Ischemic Encephalopathy in the Neonate at Birth
- PMID: 27607878
- PMCID: PMC5895085
- DOI: 10.1097/AOG.0000000000001631
Distinguishing Arterial Ischemic Stroke From Hypoxic-Ischemic Encephalopathy in the Neonate at Birth
Abstract
Objective: To identify perinatal risk factors that can distinguish arterial ischemic stroke from hypoxic-ischemic encephalopathy at birth.
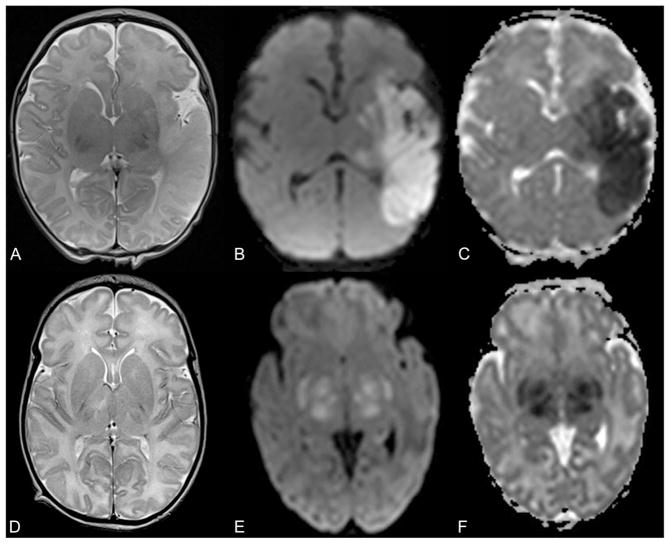
Methods: This is a cohort study of all neonates born at 35 weeks of gestation or greater admitted to our neonatal intensive care unit from January 1, 2010, to December 31, 2015, that compares neonates with stroke with those with hypoxic-ischemic encephalopathy undergoing whole-body hypothermia with abnormal brain magnetic resonance imaging.
Results: During this 6-year period, there were 22 neonates with stroke and 47 with hypoxic-ischemic encephalopathy undergoing whole-body hypothermia with abnormal magnetic resonance imaging. Three neonates triaged to hypothermia initially thought to have hypoxic-ischemic encephalopathy were later diagnosed with stroke. All neonates with stroke had a negative thrombophilia workup. Neonates with stroke had a significantly higher incidence of seizures and increased initial platelet counts on univariate analysis. A multivariable model of variables with P<.1 on univariate analysis present within 6 hours of birth found significant increases in nonreassuring fetal heart rate tracings, sentinel events, low Apgar score at 5 minutes, and metabolic acidosis at birth with hypoxic-ischemic encephalopathy. Stroke was associated with a significantly increased initial platelet count.
Conclusion: Stroke is associated with increased initial platelet counts and is not associated with cesarean delivery for nonreassuring fetal heart rate tracings, sentinel events, or perinatal metabolic acidosis. Stroke is a form of neonatal brain injury not associated with perinatal risk factors that allow early identification.
Figures
Comment in
-
Distinguishing Arterial Ischemic Stroke From Hypoxic-Ischemic Encephalopathy in the Neonate at Birth.Obstet Gynecol. 2017 Feb;129(2):388-389. doi: 10.1097/AOG.0000000000001884. Obstet Gynecol. 2017. PMID: 28121822 No abstract available.
-
In Reply.Obstet Gynecol. 2017 Feb;129(2):389-390. doi: 10.1097/AOG.0000000000001885. Obstet Gynecol. 2017. PMID: 28121823 No abstract available.
References
-
- Raju TN, Nelson KB, Ferriero D, Lynch JK NICHD-NINDS Perinatal Stroke Workshop Participants. Ischemic perinatal stroke: summary of a workshop sponsored by the National Institute of Child Health and Human Development and the National Institute of Neurological Disorders and Stroke. Pediatrics. 2007;120:609–16. - PubMed
-
- Schneider AT, Kissela B, Woo D, Kleindorfer D, Alwell K, Miller R, et al. Ischemic stroke subtypes: a population-based study of incidence rates among blacks and whites. Stroke. 2004;35:1552–6. - PubMed
-
- Kirton A, Armstrong-wells J, Chang T, Deveber G, Rivkin MJ, Hernandez M, et al. Symptomatic neonatal arterial ischemic stroke: the International Pediatric Stroke Study. Pediatrics. 2011;128:e1402–10. - PubMed
-
- Sarnat HB, Sarnat MS. Neonatal encephalopathy following fetal distress. A clinical and electroencephalographic study. Arch Neurol. 1976;33:696–705. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
