

Intentional Laceration of the Anterior Mitral Valve Leaflet to Prevent Left Ventricular Outflow Tract Obstruction During Transcatheter Mitral Valve Replacement: Pre-Clinical Findings
- PMID: 27609260
- PMCID: PMC5476960
- DOI: 10.1016/j.jcin.2016.06.020
Intentional Laceration of the Anterior Mitral Valve Leaflet to Prevent Left Ventricular Outflow Tract Obstruction During Transcatheter Mitral Valve Replacement: Pre-Clinical Findings
Abstract
Objectives: The authors propose a novel transcatheter transection of the anterior mitral leaflet to prevent iatrogenic left ventricular outflow tract (LVOT) obstruction during transcatheter mitral valve replacement (TMVR).
Background: LVOT obstruction is a life-threatening complication of TMVR caused by septal displacement of the anterior mitral leaflet.
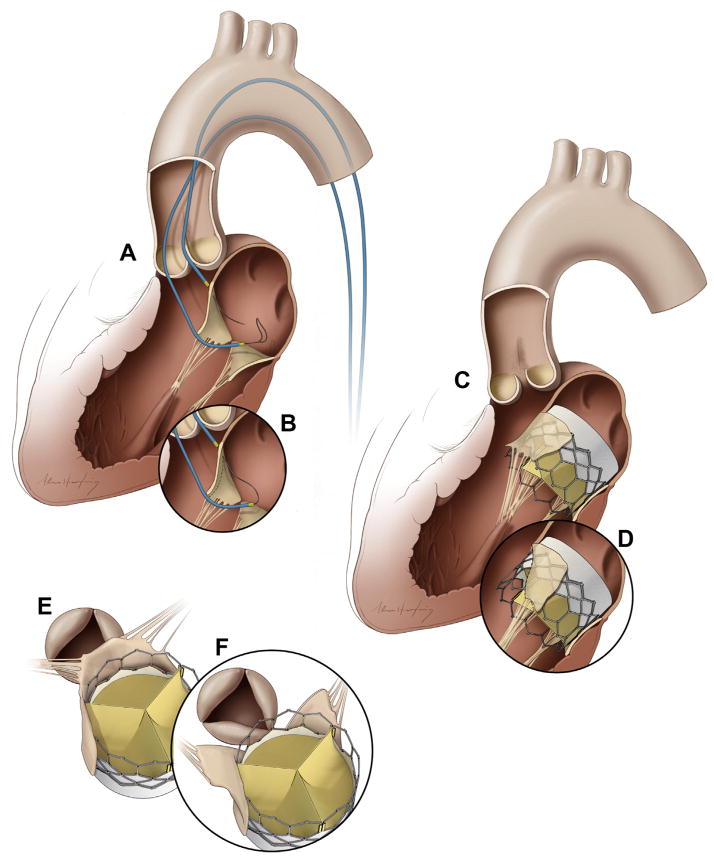
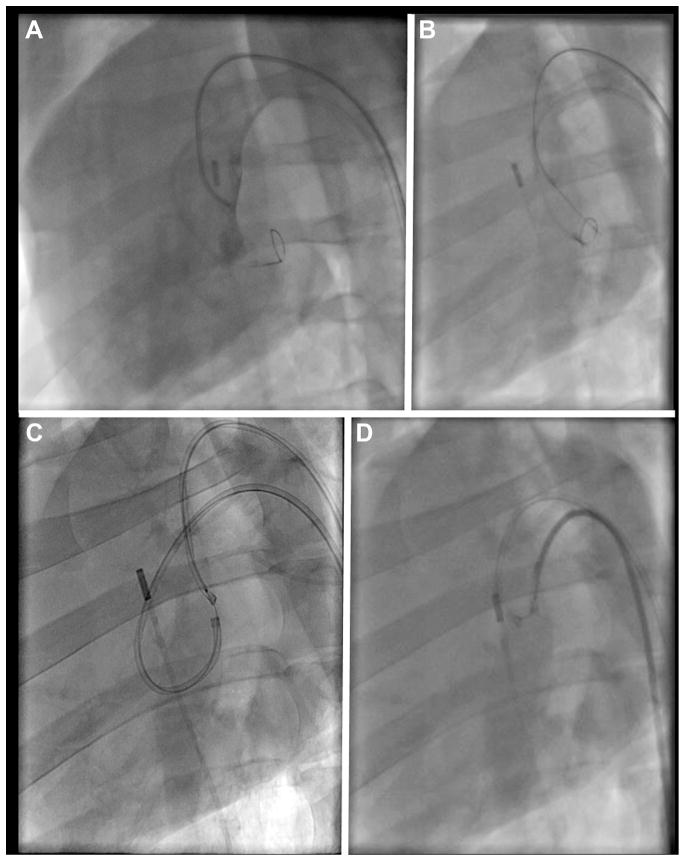
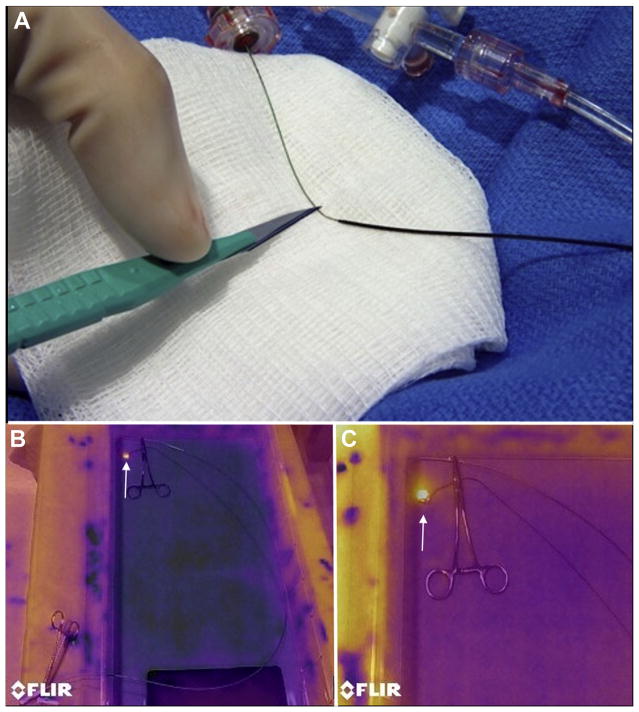
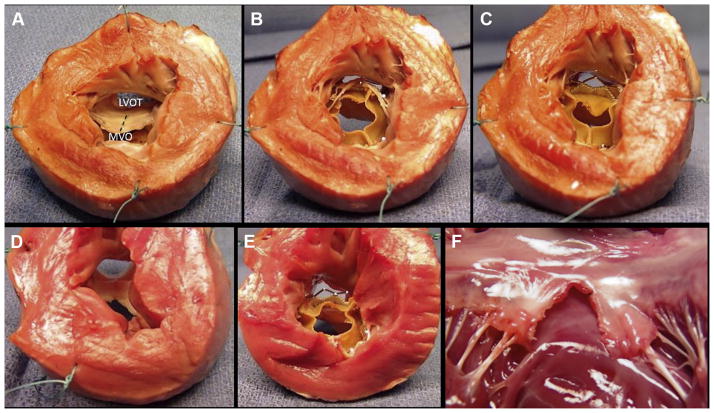
Methods: In vivo procedures in swine were guided by biplane x-ray fluoroscopy and intracardiac echocardiography. Retrograde transaortic 6-F guiding catheters straddled the anterior mitral leaflet. A stiff 0.014-inch guidewire with polymer jacket insulation was electrified and advanced from the LVOT, through the A2 leaflet base, into the left atrium. The wire was snared and externalized, forming a loop that was energized and withdrawn to lacerate the anterior mitral leaflet.
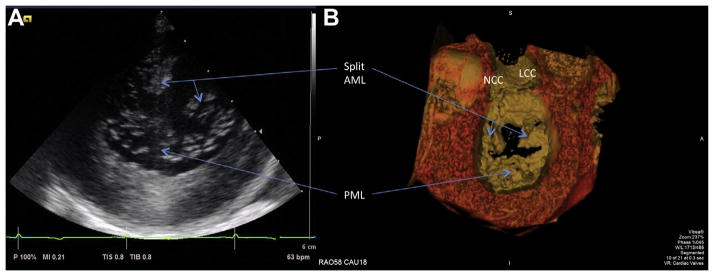
Results: The anterior mitral leaflet was successfully lacerated in 7 live and 1 post-mortem swine under heparinization. Lacerations extended to 89 ± 19% of leaflet length and were located within 0.5 ± 0.4 mm of leaflet centerline. The chordae were preserved and retracted the leaflet halves away from the LVOT. LVOT narrowing after benchtop TMVR was significantly reduced with intentional laceration of the anterior mitral leaflet to prevent LVOT obstruction than without (65 ± 10% vs. 31 ± 18% of pre-implantation diameter, p < 0.01). The technique caused mean blood pressure to fall (from 54 ± 6 mm Hg to 30 ± 4 mm Hg, p < 0.01), but blood pressure remained steady until planned euthanasia. No collateral tissue injury was identified on necropsy.
Conclusions: Using simple catheter techniques, the anterior mitral valve leaflet was transected. Cautiously applied in patients, this strategy can prevent anterior mitral leaflet displacement and LVOT obstruction caused by TMVR.
Keywords: left ventricular outflow tract obstruction; mitral valve; structural heart disease; subvalvular aortic stenosis; transcatheter mitral valve replacement; valvular heart disease.
Copyright © 2016 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Eleid MF, Cabalka AK, Williams MR, et al. Percutaneous transvenous transseptal trans-catheter valve implantation in failed bioprosthetic mitral valves, ring annuloplasty, and severe mitral annular calcification. J Am Coll Cardiol Intv. 2016;9:1161–74.
-
- Sud K, Agarwal S, Parashar A, et al. Degenerative mitral stenosis: unmet need for percutaneous interventions. Circulation. 2016;133:1594–604. - PubMed
-
- Lee KS, Stewart WJ, Lever HM, Underwood PL, Cosgrove DM. Mechanism of outflow tract obstruction causing failed mitral valve repair. Anterior displacement of leaflet coaptation. Circulation. 1993;88:II24–9. - PubMed
-
- Mihaileanu S, Marino JP, Chauvaud S, et al. Left ventricular outflow obstruction after mitral valve repair (Carpentier’s technique). Proposed mechanisms of disease. Circulation. 1988;78:I78–84. - PubMed
-
- Blanke P, Naoum C, Dvir D, et al. Predicting LVOT obstruction in transcatheter mitral valve implantation: concept of the neo-LVOT. J Am Coll Cardiol Img. In press.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
