

Rheumatoid arthritis-associated autoantibodies and subclinical interstitial lung disease: the Multi-Ethnic Study of Atherosclerosis
- PMID: 27609750
- PMCID: PMC5342945
- DOI: 10.1136/thoraxjnl-2016-208932
Rheumatoid arthritis-associated autoantibodies and subclinical interstitial lung disease: the Multi-Ethnic Study of Atherosclerosis
Abstract
Background: Adults with interstitial lung disease (ILD) often have serologic evidence of autoimmunity of uncertain significance without overt autoimmune disease. We examined associations of rheumatoid arthritis (RA)-associated antibodies with subclinical ILD in community-dwelling adults.
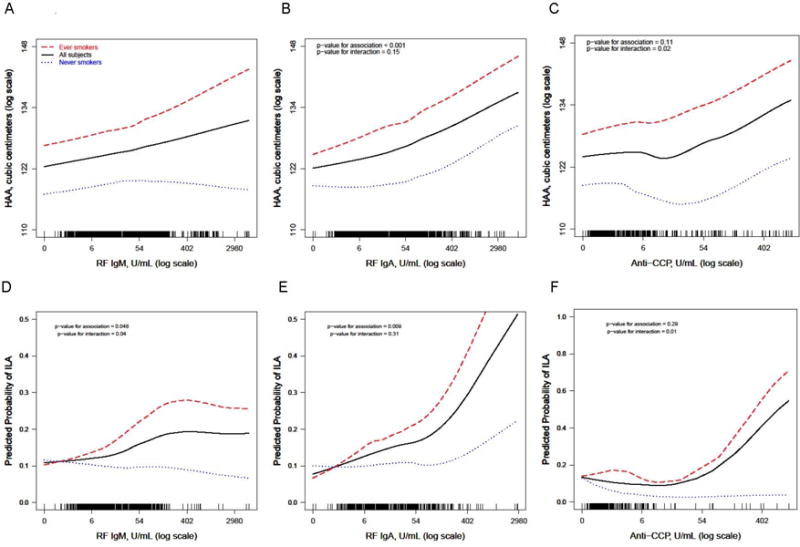
Methods: We measured serum rheumatoid factor (RF) and anticyclic citrullinated peptide antibody (anti-CCP) and high attenuation areas (HAAs; CT attenuation values between -600 and -250 Hounsfield units) on cardiac CT in 6736 community-dwelling US adults enrolled in the Multi-Ethnic Study of Atherosclerosis. We measured interstitial lung abnormalities (ILAs) in 2907 full-lung CTs at 9.5-year median follow-up. We used generalised linear and additive models to examine associations between autoantibodies and both HAA and ILA, and tested for effect modification by smoking.
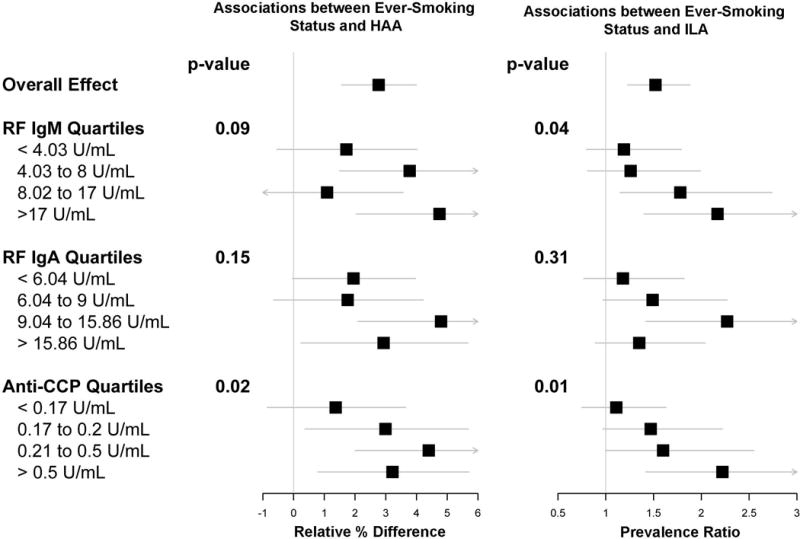
Results: In adjusted models, HAA increased by 0.49% (95% CI 0.11% to 0.86%) per doubling of RF IgM and by 0.95% (95% CI 0.50% to 1.40%) per RF IgA doubling. ILA prevalence increased by 11% (95% CI 3% to 20%) per RF IgA doubling. Smoking modified the associations of both RF IgM and anti-CCP with both HAA and ILA (interaction p values varied from 0.01 to 0.09). Among ever smokers, HAA increased by 0.81% (95% CI 0.33% to 1.30%) and ILA prevalence increased by 14% (95% CI 5% to 24%,) per RF IgM doubling; and HAA increased by 1.31% (95% CI 0.45% to 2.18%) and ILA prevalence increased by 13% (95% CI 2% to 24%) per anti-CCP doubling. Among never smokers, no meaningful associations were detected.
Conclusions: RA-related autoimmunity is associated with both quantitative and qualitative subclinical ILD phenotypes on CT, particularly among ever smokers.
Keywords: Clinical Epidemiology; Connective tissue disease associated lung disease; Interstitial Fibrosis; Rheumatoid lung disease.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/.
Conflict of interest statement
Competing interests: DJL has received consulting fees from Genentech/Roche, Boehringer-Ingelheim, Gilead, Pharmakea, Veracyte, Patara Pharmaceuticals, Degge Group and the France Foundation related to IPF; Columbia University has received funding for clinical trials in IPF from Boehringer-Ingelheim, Gilead, Bayer, Global Blood Therapeutics and Fibrogen; Columbia University has received funding from the Pulmonary Fibrosis Foundation for DJL's consulting services; DJL has received fees for serving as a Deputy Editor for the Annals of the American Thoracic Society and as a Statistical Editor for Thorax. EAH is a founder and shareholder in VIDA Diagnostics. JDN is a consultant for VIDA Diagnostics and GSK; he is also a patent holder with and has stock options in VIDA Diagnostics. JRW is a member of the IPF Rally Educational Advisory Board and has received honoraria and travel expenses from the IPF Rally Educational Advisory Board.
Figures
References
-
- Mittoo S, Gelber AC, Christopher-Stine L, et al. Ascertainment of collagen vascular disease in patients presenting with interstitial lung disease. Respir Med. 2009;103:1152–8. - PubMed
-
- Sato T, Fujita J, Yamadori I, et al. Non-specific interstitial pneumonia; as the first clinical presentation of various collagen vascular disorders. Rheumatol Int. 2006;26:551–5. - PubMed
-
- Fischer A, Antoniou KM, Brown KK, et al. An official European Respiratory Society/American Thoracic Society research statement: interstitial pneumonia with autoimmune features. Eur Respir J. 2015;46:976–87. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- N01 HC095161/HL/NHLBI NIH HHS/United States
- N01 HC095164/HC/NHLBI NIH HHS/United States
- RC1 HL100543/HL/NHLBI NIH HHS/United States
- N01 HC095160/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- R01 HL093081/HL/NHLBI NIH HHS/United States
- N01 HC095163/HL/NHLBI NIH HHS/United States
- N01 HC095165/HC/NHLBI NIH HHS/United States
- UL1 TR000040/TR/NCATS NIH HHS/United States
- N01 HC095163/HC/NHLBI NIH HHS/United States
- R01 HL104047/HL/NHLBI NIH HHS/United States
- UL1 TR001079/TR/NCATS NIH HHS/United States
- R01 HL112986/HL/NHLBI NIH HHS/United States
- R01 HL077612/HL/NHLBI NIH HHS/United States
- N01 HC095161/HC/NHLBI NIH HHS/United States
- N01 HC095162/HL/NHLBI NIH HHS/United States
- K24 HL131937/HL/NHLBI NIH HHS/United States
- R01 HL103676/HL/NHLBI NIH HHS/United States
- N01 HC095162/HC/NHLBI NIH HHS/United States
- N01 HC095165/HL/NHLBI NIH HHS/United States
- K24 HL103844/HL/NHLBI NIH HHS/United States
- N01 HC095164/HL/NHLBI NIH HHS/United States
- N01 HC095159/HC/NHLBI NIH HHS/United States
- N01 HC095160/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous