

Immediate Antiretroviral Therapy Reduces Risk of Infection-Related Cancer During Early HIV Infection
- PMID: 27609756
- PMCID: PMC5146718
- DOI: 10.1093/cid/ciw621
Immediate Antiretroviral Therapy Reduces Risk of Infection-Related Cancer During Early HIV Infection
Abstract
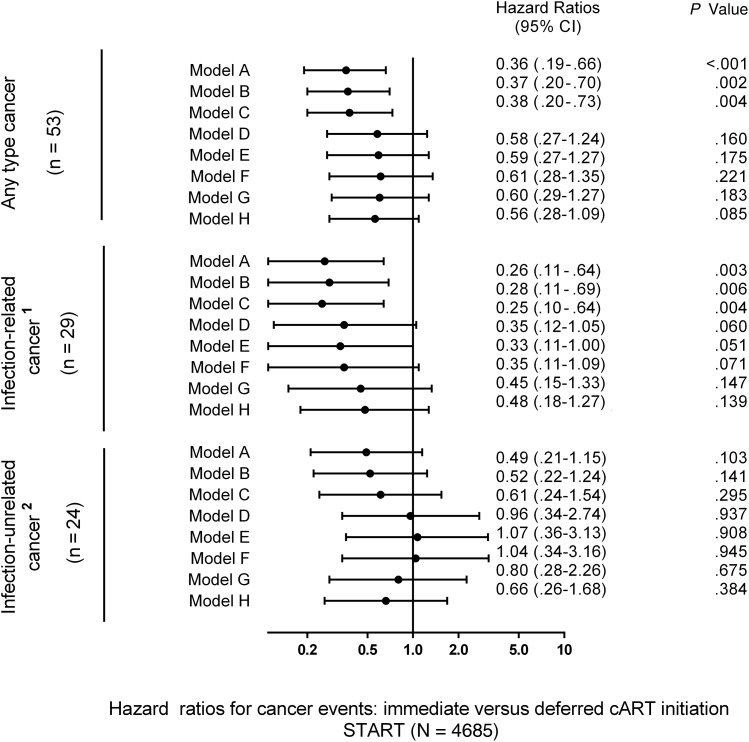
Background: In the Strategic Timing of Antiretroviral Treatment (START) study, immediate combination antiretroviral therapy (cART) initiation reduced cancer risk by 64%. We hypothesized that risk reduction was higher for infection-related cancer and determined by differences in CD4 cell counts and human immunodeficiency virus (HIV) RNA between the study arms.
Methods: Incident malignancies in START were categorized into infection-related and infection-unrelated cancer. We used Cox models to assess factors associated with both cancer categories. We used sequential adjustment for baseline covariates, cancer risk factors, and HIV-specific variables to investigate potential mediators of cancer risk reduction with immediate cART.
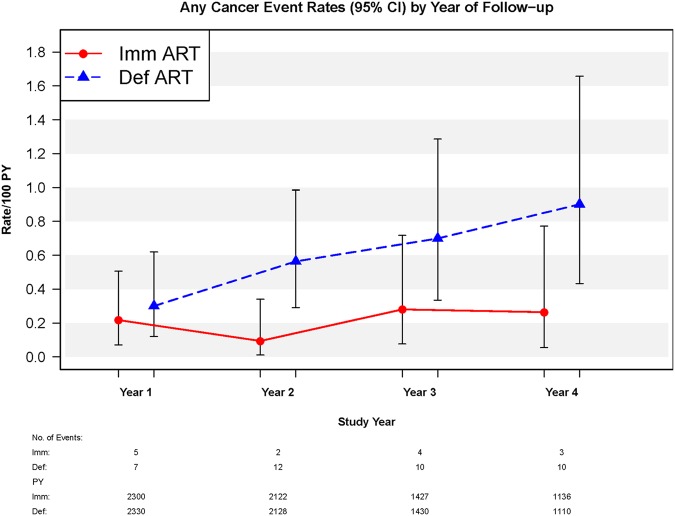
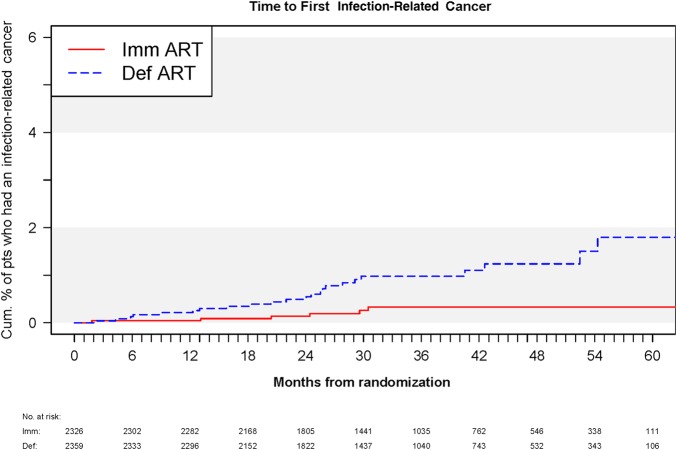
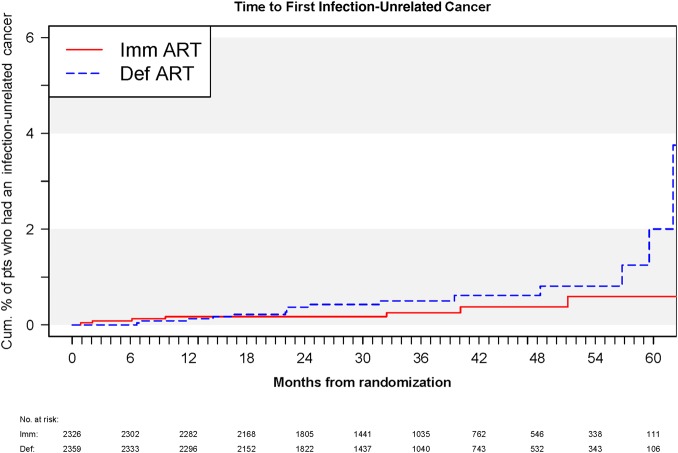
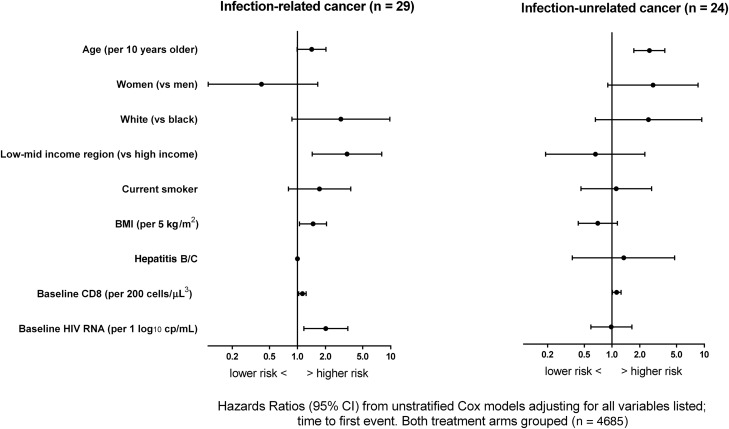
Results: There were 14 cancers among persons randomized to immediate cART (6 infection-related and 8 infection-unrelated) and 39 cancers in the deferred arm (23 infection-related and 16 infection-unrelated); hazard ratios of immediate vs deferred cART initiation were 0.26 (95% confidence interval [CI], .11-.64) for infection-related and 0.49 (95% CI, .21-1.15) for infection-unrelated cancer. Independent predictors of infection-related cancer were older age, higher body mass index, low- to middle-income region, HIV RNA, and baseline CD8 cell count. Older age and baseline CD8 cell count were independent predictors of infection-unrelated cancer. Adjustment for latest HIV RNA level had little impact on the protective effect of immediate cART on infection-related cancer. Adjustment for latest HIV RNA level, but not for CD4 cell count or cancer risk factors, attenuated the effect of immediate cART on infection-unrelated cancer.
Conclusions: Immediate cART initiation significantly reduces risk of cancer. Although limited by small sample size, this benefit does not appear to be solely attributable to HIV RNA suppression and may be also mediated by other mechanisms.
Keywords: HIV; Kaposi sarcoma; antiretroviral therapy; cancer; non-Hodgkin lymphoma.
© The Author 2016. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail journals.permissions@oup.com.
Figures
Comment in
-
Cancer Incidence in Persons Living With HIV.Clin Infect Dis. 2017 Feb 1;64(3):388-389. doi: 10.1093/cid/ciw759. Epub 2016 Nov 14. Clin Infect Dis. 2017. PMID: 28013260 No abstract available.
-
Reply to Meijide et al.Clin Infect Dis. 2017 Feb 1;64(3):389-390. doi: 10.1093/cid/ciw760. Epub 2016 Nov 14. Clin Infect Dis. 2017. PMID: 28013262 No abstract available.
References
-
- Clifford GM, Polesel J, Rickenbach M et al. . Cancer risk in the Swiss HIV Cohort Study: associations with immunodeficiency, smoking, and highly active antiretroviral therapy. J Natl Cancer Inst 2005; 97:425–32. - PubMed
-
- Guiguet M, Boué F, Cadranel J et al. . Effect of immunodeficiency, HIV viral load, and antiretroviral therapy on the risk of individual malignancies (FHDH-ANRS CO4): a prospective cohort study. Lancet Oncol 2009; 10:1152–9. - PubMed
-
- Reekie J, Kosa C, Engsig F et al. . Relationship between current level of immunodeficiency and non-acquired immunodeficiency syndrome-defining malignancies. Cancer 2010; 116:5306–15. - PubMed
-
- Helleberg M, Gerstoft J, Afzal S et al. . Risk of cancer among HIV-infected individuals compared to the background population: impact of smoking and HIV. AIDS 2014; 28:1499–508. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
