

Multivariable fractional polynomial interaction to investigate continuous effect modifiers in a meta-analysis on higher versus lower PEEP for patients with ARDS
- PMID: 27609843
- PMCID: PMC5020750
- DOI: 10.1136/bmjopen-2016-011148
Multivariable fractional polynomial interaction to investigate continuous effect modifiers in a meta-analysis on higher versus lower PEEP for patients with ARDS
Abstract
Objectives: A recent individual patient data (IPD) meta-analysis suggested that patients with moderate or severe acute respiratory distress syndrome (ARDS) benefit from higher positive end-expiratory pressure (PEEP) ventilation strategies. However, thresholds for continuous variables (eg, hypoxaemia) are often arbitrary and linearity assumptions in regression approaches may not hold; the multivariable fractional polynomial interaction (MFPI) approach can address both problems. The objective of this study was to apply the MFPI approach to investigate interactions between four continuous patient baseline variables and higher versus lower PEEP on clinical outcomes.
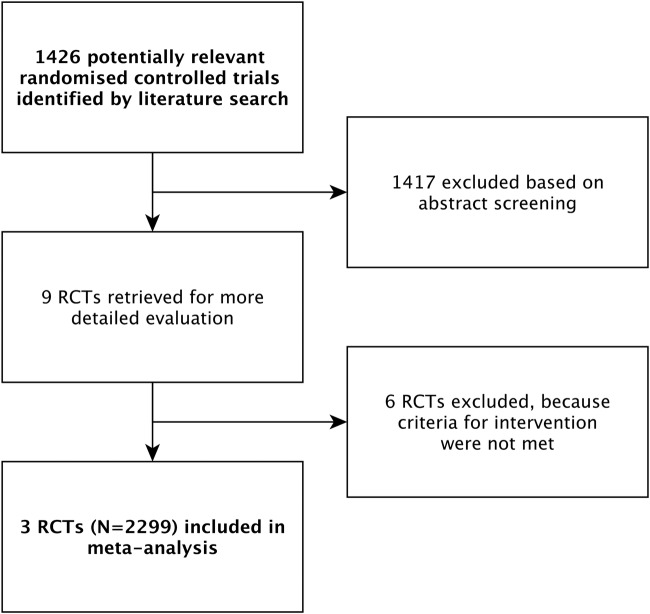
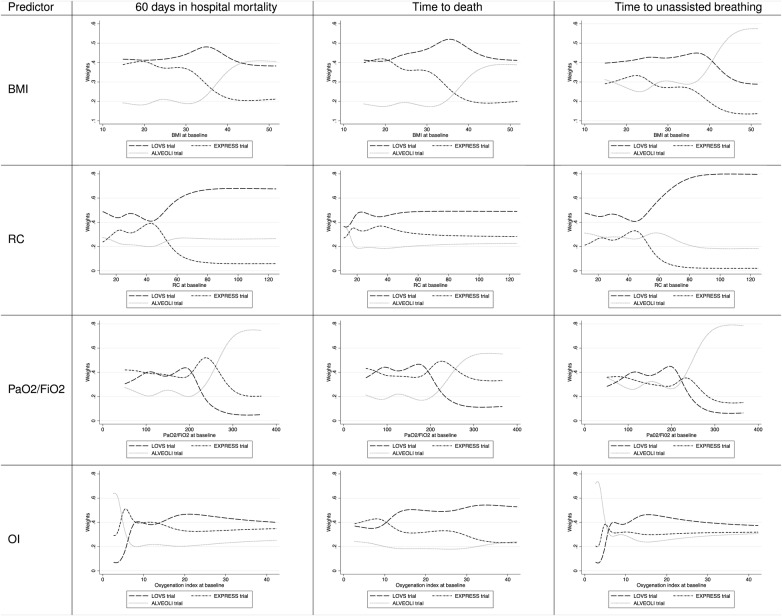
Setting: Pooled data from three randomised trials in intensive care identified by a systematic review.
Participants: 2299 patients with acute lung injury requiring mechanical ventilation.
Interventions: Higher (N=1136) versus lower PEEP (N=1163) ventilation strategy.
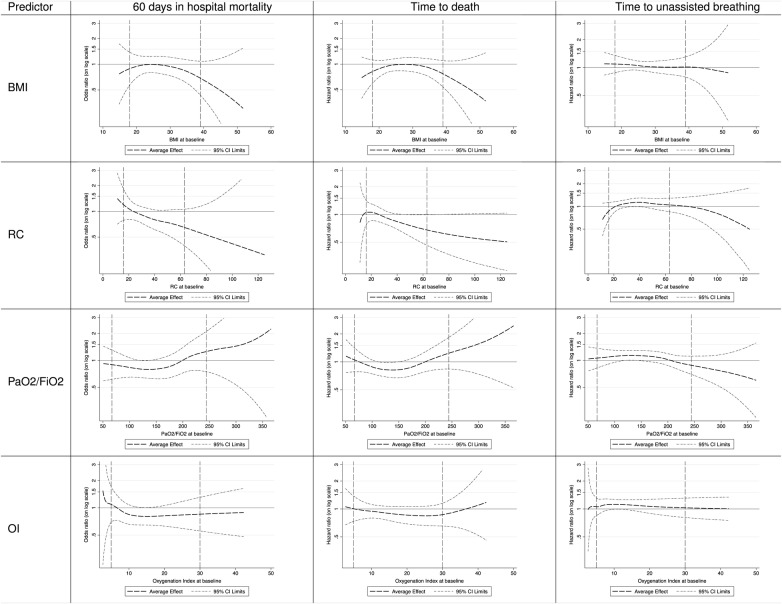
Outcome measures: Prespecified outcomes included mortality, time to death and time-to-unassisted breathing. We examined the following continuous baseline characteristics as potential effect modifiers using MFPI: PaO2/FiO2 (arterial partial oxygen pressure/ fraction of inspired oxygen), oxygenation index, respiratory system compliance (tidal volume/(inspiratory plateau pressure-PEEP)) and body mass index (BMI).
Results: We found that for patients with PaO2/FiO2 below 150 mm Hg, but above 100 mm Hg or an oxygenation index above 12 (moderate ARDS), higher PEEP reduces hospital mortality, but the beneficial effect appears to level off for patients with very severe ARDS. Patients with mild ARDS (PaO2/FiO2 above 200 mm Hg or an oxygenation index below 10) do not seem to benefit from higher PEEP and might even be harmed. For patients with a respiratory system compliance above 40 mL/cm H2O or patients with a BMI above 35 kg/m(2), we found a trend towards reduced mortality with higher PEEP, but there is very weak statistical confidence in these findings.
Conclusions: MFPI analyses suggest a nonlinear effect modification of higher PEEP ventilation by PaO2/FiO2 and oxygenation index with reduced mortality for some patients suffering from moderate ARDS.
Study registration number: CRD42012003129.
Keywords: ARDS; IPD meta-analysis; acute lung injury; multivariable fractional polynomials; treatment interaction.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Similar articles
-
Gas exchange and lung mechanics in patients with acute respiratory distress syndrome: comparison of three different strategies of positive end expiratory pressure selection.J Crit Care. 2015 Apr;30(2):334-40. doi: 10.1016/j.jcrc.2014.11.019. Epub 2014 Dec 3. J Crit Care. 2015. PMID: 25577132
-
A clinical classification of the acute respiratory distress syndrome for predicting outcome and guiding medical therapy*.Crit Care Med. 2015 Feb;43(2):346-53. doi: 10.1097/CCM.0000000000000703. Crit Care Med. 2015. PMID: 25393701
-
A high positive end-expiratory pressure, low tidal volume ventilatory strategy improves outcome in persistent acute respiratory distress syndrome: a randomized, controlled trial.Crit Care Med. 2006 May;34(5):1311-8. doi: 10.1097/01.CCM.0000215598.84885.01. Crit Care Med. 2006. PMID: 16557151 Clinical Trial.
-
Acute Respiratory Distress Syndrome: Advances in Diagnosis and Treatment.JAMA. 2018 Feb 20;319(7):698-710. doi: 10.1001/jama.2017.21907. JAMA. 2018. PMID: 29466596 Review.
-
Lung recruitment maneuvers in acute respiratory distress syndrome and facilitating resolution.Crit Care Med. 2003 Apr;31(4 Suppl):S265-71. doi: 10.1097/01.CCM.0000057902.29449.29. Crit Care Med. 2003. PMID: 12682451 Review.
Cited by
-
Airway Pressure Release Ventilation Mode Improves Circulatory and Respiratory Function in Patients After Cardiopulmonary Bypass, a Randomized Trial.Front Physiol. 2021 Jun 3;12:684927. doi: 10.3389/fphys.2021.684927. eCollection 2021. Front Physiol. 2021. PMID: 34149459 Free PMC article.
-
Nonlinear effects and effect modification at the participant-level in IPD meta-analysis part 2: methodological guidance is available.J Clin Epidemiol. 2023 Jul;159:319-329. doi: 10.1016/j.jclinepi.2023.04.014. Epub 2023 May 3. J Clin Epidemiol. 2023. PMID: 37146657 Free PMC article.
-
Nonlinear effects and effect modification at the participant-level in IPD meta-analysis part 1: analysis methods are often substandard.J Clin Epidemiol. 2023 Jul;159:309-318. doi: 10.1016/j.jclinepi.2023.04.013. Epub 2023 May 4. J Clin Epidemiol. 2023. PMID: 37146661 Free PMC article.
-
Individual participant data meta-analysis to examine interactions between treatment effect and participant-level covariates: Statistical recommendations for conduct and planning.Stat Med. 2020 Jul 10;39(15):2115-2137. doi: 10.1002/sim.8516. Epub 2020 Apr 30. Stat Med. 2020. PMID: 32350891 Free PMC article.
-
Unusual Localization of Blood-Borne Loa loa Microfilariae in the Skin Depends on Microfilarial Density in the Blood: Implications for Onchocerciasis Diagnosis in Coendemic Areas.Clin Infect Dis. 2021 Jun 14;72(Suppl 3):S158-S164. doi: 10.1093/cid/ciab255. Clin Infect Dis. 2021. PMID: 33909066 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources