

Cost-efficiency of specialist hyperacute in-patient rehabilitation services for medically unstable patients with complex rehabilitation needs: a prospective cohort analysis
- PMID: 27609852
- PMCID: PMC5020841
- DOI: 10.1136/bmjopen-2016-012112
Cost-efficiency of specialist hyperacute in-patient rehabilitation services for medically unstable patients with complex rehabilitation needs: a prospective cohort analysis
Abstract
Objectives: To evaluate functional outcomes, care needs and cost-efficiency of hyperacute (HA) rehabilitation for a cohort of in-patients with complex neurological disability and unstable medical/surgical conditions.
Design: A multicentre cohort analysis of prospectively collected clinical data from the UK Rehabilitation Outcomes Collaborative (UKROC) national clinical database, 2012-2015.
Setting: Two HA specialist rehabilitation services in England, providing different service models for HA rehabilitation.
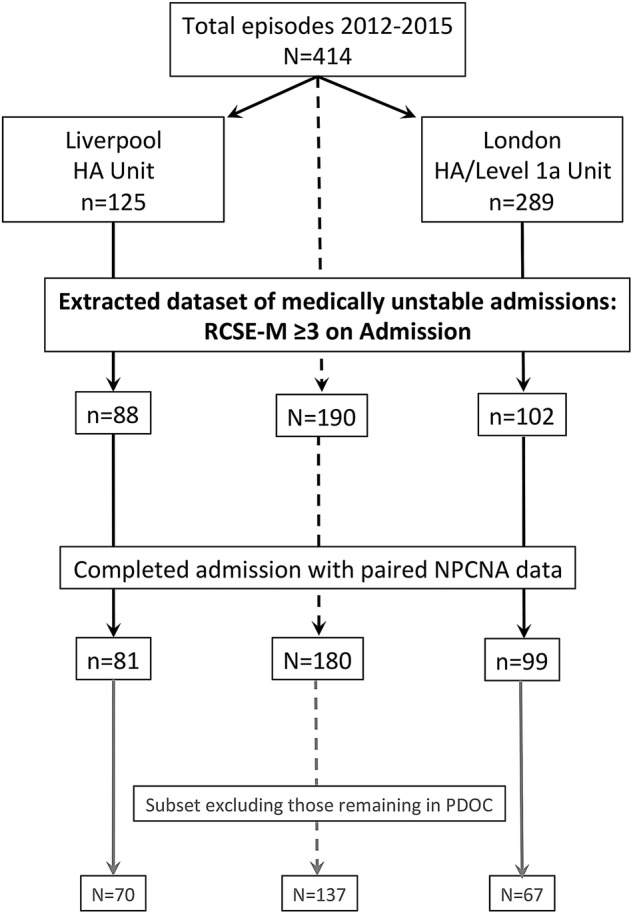
Participants: All patients admitted to each of the units with an admission rehabilitation complexity M score of ≥3 (N=190; mean age 46 (SD16) years; males:females 63:37%). Diagnoses were acquired brain injury (n=166; 87%), spinal cord injury (n=9; 5%), peripheral neurological conditions (n=9; 5%) and other (n=6; 3%).
Intervention: Specialist in-patient multidisciplinary rehabilitation combined with management and stabilisation of intercurrent medical and surgical problems.
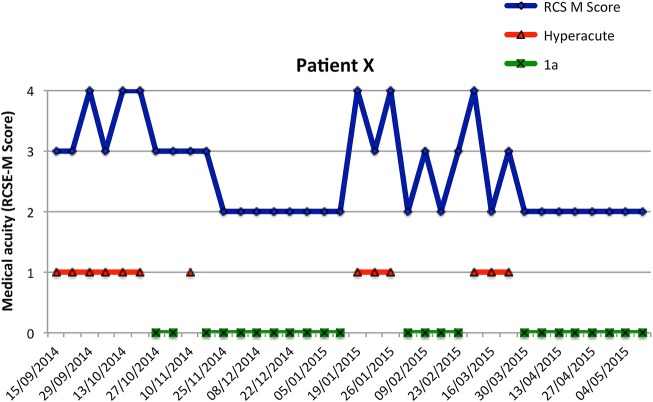
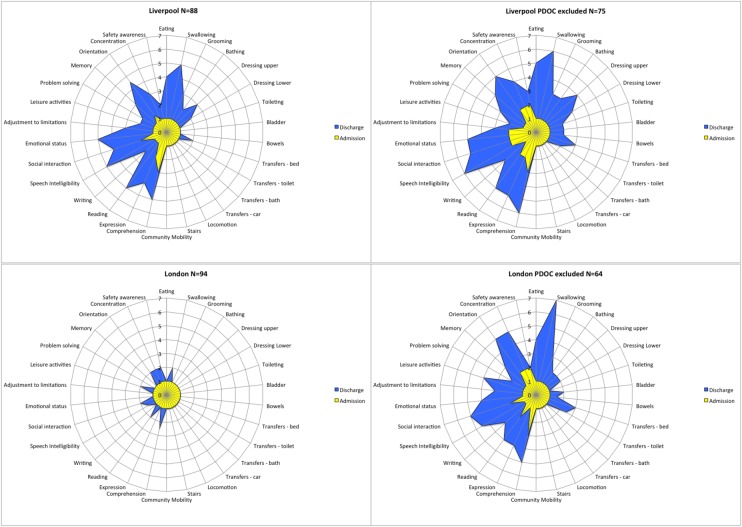
Outcome measures: Rehabilitation complexity and medical acuity: Rehabilitation Complexity Scale-version 13. Dependency and care costs: Northwick Park Dependency Scale/Care Needs Assessment (NPDS/NPCNA). Functional independence: UK Functional Assessment Measure (UK FIM+FAM).
Primary outcomes: (1) reduction in dependency and (2) cost-efficiency, measured as the time taken to offset rehabilitation costs by savings in NPCNA-estimated costs of on-going care in the community.
Results: The mean length of stay was 103 (SD66) days. Some differences were observed between the two units, which were in keeping with the different service models. However, both units showed a significant reduction in dependency and acuity between admission and discharge on all measures (Wilcoxon: p<0.001). For the 180 (95%) patients with complete NPCNA data, the mean episode cost was £77 119 (bootstrapped 95% CI £70 614 to £83 894) and the mean reduction in 'weekly care costs' was £462/week (95% CI 349 to 582). The mean time to offset the cost of rehabilitation was 27.6 months (95% CI 13.2 to 43.8).
Conclusions: Despite its relatively high initial cost, specialist HA rehabilitation can be highly cost-efficient, producing substantial savings in on-going care costs, and relieving pressure in the acute care services.
Keywords: Cost-efficiency; Functional gain; Outcome measurement.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://www.bmj.com/company/products-services/rights-and-licensing/
Figures
Similar articles
-
Cost-efficiency of specialist inpatient rehabilitation for working-aged adults with complex neurological disabilities: a multicentre cohort analysis of a national clinical data set.BMJ Open. 2016 Feb 24;6(2):e010238. doi: 10.1136/bmjopen-2015-010238. BMJ Open. 2016. PMID: 26911586 Free PMC article.
-
Functional outcomes and cost-efficiency of specialist in-patient rehabilitation following spinal cord injury: a multi-centre national cohort analysis from the UK Rehabilitation Outcomes Collaborative (UKROC).Disabil Rehabil. 2022 Sep;44(19):5603-5611. doi: 10.1080/09638288.2021.1946603. Epub 2021 Jul 20. Disabil Rehabil. 2022. PMID: 34282991
-
Cost efficiency of inpatient rehabilitation following acquired brain injury: the first international adaptation of the UK approach.BMJ Open. 2024 Dec 22;14(12):e094892. doi: 10.1136/bmjopen-2024-094892. BMJ Open. 2024. PMID: 39806612 Free PMC article.
-
Healthcare tariffs for specialist inpatient neurorehabilitation services: rationale and development of a UK casemix and costing methodology.Clin Rehabil. 2012 Mar;26(3):264-79. doi: 10.1177/0269215511417467. Epub 2011 Oct 4. Clin Rehabil. 2012. PMID: 21971751 Review.
-
Psychometric evaluation of the Northwick Park Dependency Scale.J Rehabil Med. 2010 Nov;42(10):936-43. doi: 10.2340/16501977-0602. J Rehabil Med. 2010. PMID: 21031290 Review.
Cited by
-
Management of traumatic brain injury (TBI): a clinical neuroscience-led pathway for the NHS.Clin Med (Lond). 2021 Mar;21(2):e198-e205. doi: 10.7861/clinmed.2020-0336. Clin Med (Lond). 2021. PMID: 33762387 Free PMC article.
-
Caring for high-need patients.BMC Health Serv Res. 2023 Nov 23;23(1):1289. doi: 10.1186/s12913-023-10236-w. BMC Health Serv Res. 2023. PMID: 37996845 Free PMC article.
-
How Can Policymakers be Encouraged to Support People With Spinal Cord Injury-Scoping Review.Global Spine J. 2022 May;12(4):732-741. doi: 10.1177/21925682211005406. Epub 2021 Apr 20. Global Spine J. 2022. PMID: 33878912 Free PMC article.
-
Brain injury rehabilitation after road trauma in new South Wales, Australia - insights from a data linkage study.BMC Health Serv Res. 2018 Mar 23;18(1):204. doi: 10.1186/s12913-018-3019-8. BMC Health Serv Res. 2018. PMID: 29566689 Free PMC article.
-
Value and Cost Savings From Access to Multi-disciplinary Rehabilitation Services After Severe Acquired Brain Injury.Front Public Health. 2021 Dec 1;9:753447. doi: 10.3389/fpubh.2021.753447. eCollection 2021. Front Public Health. 2021. PMID: 34926379 Free PMC article.
References
-
- Turner-Stokes L, Nair A, Disler P et al. . Multi-disciplinary rehabilitation for acquired brain injury in adults of working age. Cochrane Database Syst Rev 2005;(3):CD004170 (Updated 2015). - PubMed
-
- Major Trauma Services: D15 Service Specification. London 2013 (cited 2014). http://www.england.nhs.uk/wp-content/uploads/2014/04/d02-rehab-pat-high-....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical