

Alcohol, Cannabis, and Opioid Use Disorders, and Disease Burden in an Integrated Health Care System
- PMID: 27610582
- PMCID: PMC5291754
- DOI: 10.1097/ADM.0000000000000260
Alcohol, Cannabis, and Opioid Use Disorders, and Disease Burden in an Integrated Health Care System
Abstract
Objectives: We examined prevalence of major medical conditions and extent of disease burden among patients with and without substance use disorders (SUDs) in an integrated health care system serving 3.8 million members.
Methods: Medical conditions and SUDs were extracted from electronic health records in 2010. Patients with SUDs (n = 45,461; alcohol, amphetamine, barbiturate, cocaine, hallucinogen, and opioid) and demographically matched patients without SUDs (n = 45,461) were compared on the prevalence of 19 major medical conditions. Disease burden was measured as a function of 10-year mortality risk using the Charlson Comorbidity Index. P-values were adjusted using Hochberg's correction for multiple-inference testing within each medical condition category.
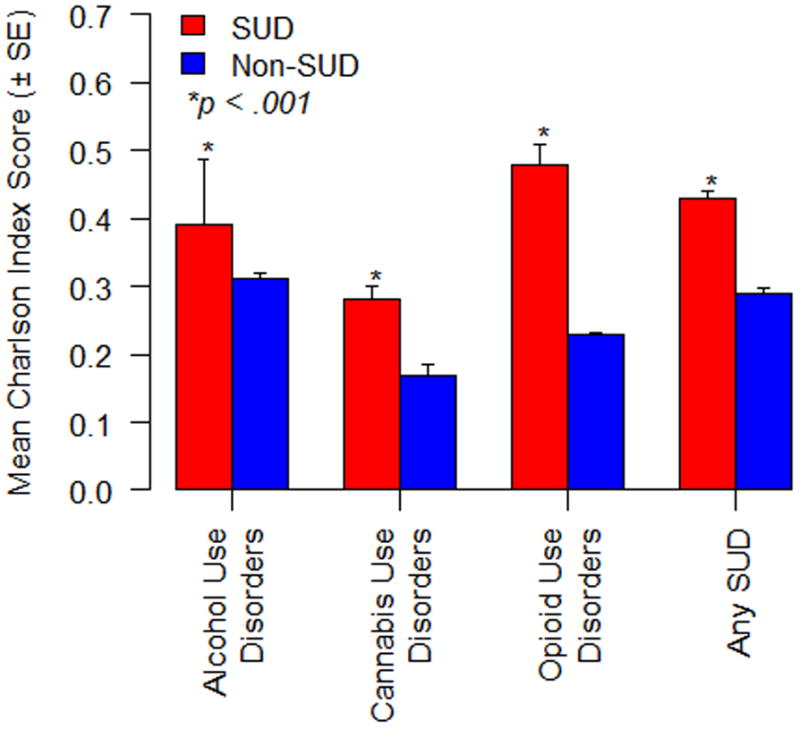
Results: The most frequently diagnosed SUDs in 2010 were alcohol (57.6%), cannabis (14.9%), and opioid (12.9%). Patients with these SUDs had higher prevalence of major medical conditions than non-SUD patients (alcohol use disorders, 85.3% vs 55.3%; cannabis use disorders, 41.9% vs 23.0%; and opioid use disorders, 44.9% vs 26.1%; all P < 0.001). Patients with these SUDs also had higher disease burden than non-SUD patients; patients with opioid use disorders (M = 0.48; SE = 1.46) had particularly high disease burden (M = 0.23; SE = 0.09; P < 0.001).
Conclusions: Common SUDs, particularly opioid use disorders, are associated with substantial disease burden for privately insured individuals without significant impediments to care. This signals the need to explore the full impact SUDs have on the course and outcome of prevalent conditions and initiate enhanced service engagement strategies to improve disease burden.
Figures
References
-
- Berthiller J, Straif K, Boniol M, et al. Cannabis smoking and risk of lung cancer in men: a pooled analysis of three studies in Maghreb. J Thorac Oncol. 2008;3:1398–13403. - PubMed
-
- Birnbaum H, White A, Schiller M, Waldman T, Cleveland J, Roland C. Societal costs of prescription opioid abuse, dependence, and misuse in the United States. Pain Med. 2011;12(4):657–667. - PubMed
-
- Boyd C, Leff B, Weiss C, Wolff J, Hamblin A, Martin L. Clarifying multi-morbidity patterns to improve targeting and delivery of clinical services for Medicaid populations. Center for Health Care Strategies. Inc.; Dec, 2010.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
