

Intravenous versus inhalational techniques for rapid emergence from anaesthesia in patients undergoing brain tumour surgery
- PMID: 27611234
- PMCID: PMC6457852
- DOI: 10.1002/14651858.CD010467.pub2
Intravenous versus inhalational techniques for rapid emergence from anaesthesia in patients undergoing brain tumour surgery
Abstract
Background: Brain tumour surgery usually is carried out with the patient under general anaesthesia. Over past years, both intravenous and inhalational anaesthetic agents have been used, but the superiority of one agent over the other is a topic of ongoing debate. Early and rapid emergence from anaesthesia is desirable for most neurosurgical patients. With the availability of newer intravenous and inhalational anaesthetic agents, all of which have inherent advantages and disadvantages, we remain uncertain as to which technique may result in more rapid early recovery from anaesthesia.
Objectives: To assess the effects of intravenous versus inhalational techniques for rapid emergence from anaesthesia in patients undergoing brain tumour surgery.
Search methods: We searched the Cochrane Central Register of Controlled Trials (CENTRAL; 2014, Issue 6) in The Cochrane Library, MEDLINE via Ovid SP (1966 to June 2014) and Embase via Ovid SP (1980 to June 2014). We also searched specific websites, such as www.indmed.nic.in, www.cochrane-sadcct.org and www.Clinicaltrials.gov (October 2014). We reran the searches for all databases in March 2016, and when we update the review, we will deal with the two studies of interest found through this search that are awaiting classification.
Selection criteria: We included randomized controlled trials (RCTs) that compared the use of intravenous anaesthetic agents such as propofol and thiopentone with inhalational anaesthetic agents such as isoflurane and sevoflurane for maintenance of general anaesthesia during brain tumour surgery. Primary outcomes were emergence from anaesthesia (assessed by time to follow verbal commands, in minutes) and adverse events during emergence, such as haemodynamic changes, agitation, desaturation, muscle weakness, nausea and vomiting, shivering and pain. Secondary outcomes were time to eye opening, recovery from anaesthesia using the Aldrete or Modified Aldrete score (i.e. time to attain score ≥ 9, in minutes), opioid consumption, brain relaxation (as assessed by the surgeon on a 4- or 5-point scale) and complications of anaesthetic techniques, such as intraoperative haemodynamic instability in terms of hypotension or hypertension (mmHg), increased or decreased heart rate (beats/min) and brain swelling.
Data collection and analysis: We used standardized methods in conducting the systematic review, as described by the Cochrane Handbook for Systematic Reviews of Interventions. Two review authors independently extracted details of trial methods and outcome data from reports of all trials considered eligible for inclusion. We performed all analyses on an intention-to-treat basis. We used a fixed-effect model when we found no evidence of significant heterogeneity between studies, and a random-effects model when heterogeneity was likely. For assessments of the overall quality of evidence for each outcome that included pooled data from RCTs only, we downgraded the evidence from 'high quality' by one level for serious (or by two levels for very serious) study limitations (risk of bias), indirectness of evidence, serious inconsistency, imprecision of effect or potential publication bias.
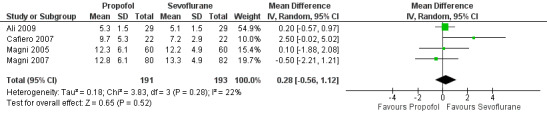
Main results: We included 15 RCTs with 1833 participants. We determined that none of the RCTs were of high methodological quality. For our primary outcomes, pooled results from two trials suggest that time to emergence from anaesthesia, that is, time needed to follow verbal commands, was longer with isoflurane than with propofol (mean difference (MD) -3.29 minutes, 95% confidence interval (CI) -5.41 to -1.18, low-quality evidence), and time to emergence from anaesthesia was not different with sevoflurane compared with propofol (MD 0.28 minutes slower with sevoflurane, 95% CI -0.56 to 1.12, four studies, low-quality evidence). Pooled analyses for adverse events suggest lower risk of nausea and vomiting with propofol than with sevoflurane (risk ratio (RR) 0.68, 95% CI 0.51 to 0.91, low-quality evidence) or isoflurane (RR 0.45, 95% CI 0.26 to 0.78) and greater risk of haemodynamic changes with propofol than with sevoflurane (RR 1.85, 95% CI 1.07 to 3.17), but no differences in the risk of shivering or pain. Pooled analyses for brain relaxation suggest lower risk of tense brain with propofol than with isoflurane (RR 0.88, 95% CI 0.67 to 1.17, low-quality evidence), but no difference when propofol is compared with sevoflurane.
Authors' conclusions: The finding of our review is that the intravenous technique is comparable with the inhalational technique of using sevoflurane to provide early emergence from anaesthesia. Adverse events with both techniques are also comparable. However, we derived evidence of low quality from a limited number of studies. Use of isoflurane delays emergence from anaesthesia. These results should be interpreted with caution. Randomized controlled trials based on uniform and standard methods are needed. Researchers should follow proper methods of randomization and blinding, and trials should be adequately powered.
Conflict of interest statement
Gyaninder Pal Singh: none known.
Hemanshu Prabhakar: none known.
Mani Kalaivani: none known.
Vidhu Anand: none known.
Charu Mahajan: none known.
Indu Kapoor: none known.
Figures














Update of
- doi: 10.1002/14651858.CD010467
References
References to studies included in this review
Ali 2009 {published data only}
-
- Ali Z, Prabhakar H, Bithal PK, Dash HH. Bispectral index‐guided administration of anesthesia for transsphenoidal resection of pituitary tumors: a comparison of 3 anesthetic techniques. Journal of Neurosurgical Anesthesiology 2009;21:10‐5. [PUBMED: 19098618] - PubMed
Banevicius 2010 {published data only}
-
- Banevicius G, Rugyte D, Macas A, Tamasauskas A, Stankevicius E. The effect of sevoflurane and propofol on cerebral hemodynamics during intracranial tumors surgery under monitoring the depth of anesthesia. Medicinas (Kaunas) 2010;46:743‐52. [PUBMED: 21467832 ] - PubMed
Bonhomme 2009 {published data only}
-
- Bonhomme V, Demoitie J, Schaub I, Hans P. Acid‐base status and hemodynamic stability during propofol and sevoflurane–based anesthesia in patients undergoing intracranial surgery. Journal of Neurosurgical Anesthesiology 2009;21:112‐9. [PUBMED: 19295389 ] - PubMed
Cafiero 2007 {published data only}
-
- Cafiero T, Cavallo LM, Frangiosa A, Burrelli R, Gargiulo G, Cappabianca P, et al. Clinical comparison of remifentanil‐sevoflurane vs. remifentanil‐propofol for endoscopic endonasal transsphenoidal surgery. European Journal of Anaesthesiology 2007;24:441‐6. [PUBMED: 17376252 ] - PubMed
Citerio 2012 {published data only}
-
- Citerio G, Pesenti A, Latini R, Masson S, Barlera S, Gaspari F, et al. for the NeuroMorfeo Study Group. A multicentre, randomised, open‐label, controlled trial evaluating equivalence of inhalational and intravenous anaesthesia during elective craniotomy. European Journal of Anaesthesiology 2012;29:371‐9. [PUBMED: 22569025 ] - PubMed
Fabregas 1995 {published data only}
-
- Fabregas N, Valero R, Carrero E, Gonzalez M, Soley R, Nalda MA. Intravenous anesthesia with propofol in neurosurgery of long duration. Revista Española de Anestesiología y Reanimación 1995;42:163‐8. [PUBMED: 7792414 ] - PubMed
Grundy 1992 {published data only}
-
- Grundy BL, Pashayan AG, Mahla ME, Shah BD. Three balanced anesthetic techniques for neuroanesthesia: infusion of thiopental sodium with sufentanil or fentanyl compared with inhalation of isoflurane. Journal of Clinical Anesthesia 1992;4:372‐7. [PUBMED: 1389190 ] - PubMed
Ittichaikulthol 1997 {published data only}
-
- Ittichaikulthol W, Pausawasdi, Srichintai P, Sarnvivad P. Propofol vs isoflurane for neurosurgical anesthesia in Thai patients. Journal of the Medical Association of Thailand=chotmaihet thangphaet 1997;80:454‐60. [PUBMED: 9277075 ] - PubMed
Lauta 2010 {published data only}
-
- Lauta E, Abbinante C, Gaudio AD, Aloj F, Fanelli M, Vivo P, et al. Emergence times are similar with sevoflurane and total intravenous anesthesia: results of a multicenter RCT of patients scheduled for elective supratentorial craniotomy. Journal of Neurosurgical Anesthesiology 2010;22:110‐8. [PUBMED: 20308817 ] - PubMed
Magni 2005 {published data only}
-
- Magni G, Baisi F, Rosa I, Imperiale C, Fabbrini V, Pennacchiotti ML, et al. No difference in emergence time and early cognitive function between sevoflurane‐fentanyl and propofol‐remifentanil in patients undergoing craniotomy for supratentorial intracranial surgery. Journal of Neurosurgical Anesthesiology 2005;17:134‐8. [PUBMED: 16037733] - PubMed
Magni 2007 {published data only}
-
- Magni G, Rosa IL, Gimignani S, Melillo G, Imperiale C, Rosa G. Early postoperative complications after intracranial surgery ‐ comparison between total intravenous and balanced anesthesia. Journal of Neurosurgical Anesthesiology 2007;19:229‐34. [PUBMED: 17893573 ] - PubMed
Petersen 2003 {published data only}
-
- Petersen KD, Landsfeldt U, Cold GE, Petersen CB, Mau S, Hauerberg J, et al. Intracranial pressure and cerebral hemodynamic in patients with cerebral tumors: a randomized prospective study of patients subjected to craniotomy in propofol‐fentanyl, isoflurane‐fentanyl, or sevoflurane‐fentanyl anesthesia. Anesthesiology 2003;98:329‐36. [PUBMED: 12552189] - PubMed
Sneyd 2005 {published data only}
-
- Sneyd JR, Andrews CJH, Tsubokawa T. Comparison of propofol/remifentanil and sevoflurane/remifentanil for maintenance of anaesthesia for elective intracranial surgery. British Journal of Anaesthesia 2005;94:778‐83. [PUBMED: 15833780 ] - PubMed
Talke 2002 {published data only}
-
- Talke P, Caldwell JE, Brown R, Dodson B, Howley J, Richardson CA. A comparison of three anaesthetic techniques in patients undergoing craniotomy for supratentorial intracranial surgery. Anesthesia and Analgesia 2002;95:430‐5. [PUBMED: 12145066 ] - PubMed
Todd 1993 {published data only}
-
- Todd MM, Warner DS, Sokoll MD, Maktabi MA, Hindman BJ, Scamman FL, et al. A prospective comparative trial of three anesthetics for elective supratentorial craniotomy. Propofol/fentanyl, isoflurane/nitrous oxide, and fentanyl/nitrous oxide. Anesthesiology 1993;78:1005‐20. [PUBMED: 8512094] - PubMed
References to studies excluded from this review
Van Aken 1990 {published data only}
-
- Aken H, Hemelrijck J, Merckx L, Möllhoff T, Mulier J, Lübbesmeyer HJ. Total intravenous anesthesia using propofol and alfentanil in comparison with balanced anesthesia in neurosurgery. Anästhesie, Intensivtherapie, Notfallmedizin 1990;25:54‐8. [PUBMED: 2309991 ] - PubMed
Van Hemelrijck 1991 {published data only}
-
- Van Hemelrijck, Aken H, Merckx L, Mulier J. Anesthesia for craniotomy: total intravenous anesthesia with propofol and alfentanil compared to anesthesia with thiopental sodium, isoflurane, fentanyl, and nitrous oxide. Journal of Clinical Anesthesia 1991;3:131‐6. [PUBMED: 2039640 ] - PubMed
Weninger 2004 {published data only}
-
- Weninger B, Czerner S, Steude U, Weninger E. Comparison between TCI‐TIVA, manual TIVA and balanced anaesthesia for stereotactic biopsy of brain. Anasthesiol Intensivmed Notfallmed Schmerzther 2004;39:212‐9. [PUBMED: 15098169 ] - PubMed
References to studies awaiting assessment
Bastola 2015 {published data only}
Necib 2014 {published data only}
-
- Necib S, Tubach F, Peuch C, LeBihan E, Samain E, Mantz J, et al. Recovery from anesthesia after craniotomy for supratentorial tumors: comparison of propofol‐remifentanil and sevoflurane‐sufentanil (the PROMIFLUNIL trial). Journal of Neurosurgical Anesthesiology 2014;26:37‐44. [PUBMED: 23774117 ] - PubMed
Additional references
Alkire1995
-
- Alkire MT, Haier RJ, Barker SJ, Shah NK, Wu JC, Kao J. Cerebral metabolism during propofol anesthesia in humans studied with positron emission tomography. Anesthesiology 1995;82:393‐403. [PUBMED: 7856898] - PubMed
Citerio 2009
Craen 1992
-
- Craen RA, Gelb AW. The anaesthetic management of neurosurgical emergencies. Canadian Journal of Anaesthesiology 1992;39(5):R29‐39. [PUBMED: 1600571] - PubMed
DerSimonian 1986
-
- DerSimonian R, Laird N. Meta‐analysis in clinical trials. Controlled Clinical Trials 1986;7:177‐88. [PUBMED: 3802833] - PubMed
Engelhard 2006
-
- Engelhard K, Werner C. Inhalational or intravenous anesthetics for craniotomies? Pro inhalational. Current Opinion in Anesthesiology 2006;19:504‐8. [PUBMED: 16960482] - PubMed
Gupta 2004
-
- Gupta A, Stierer T, Zuckerman R, Sakima N, Parker SD, Fleisher LA. Comparison of recovery profile after ambulatory anesthesia with propofol, isoflurane, sevoflurane and desflurane: a systematic review. Anesthesia and Analgesia 2004;98(3):632–41. [PUBMED: 14980911] - PubMed
Guyatt 2008
Hans 2006
-
- Hans P, Bonhomme V. Why we still use intravenous drugs as the basic regimen for neurosurgical anaesthesia. Current Opinion in Anaesthesiology 2006;19:498‐503. [PUBMED: 16960481 ] - PubMed
Higgins 2002
-
- Higgins JPT, Thompson SG. Quantifying heterogeneity in a meta‐analysis. Statistics in Medicine 2002;11(21):1539‐58. [PUBMED: 12111919] - PubMed
Higgins 2011
-
- Higgins JPT, Green S (editors). Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0 [updated March 2011]. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org.
Lefebvre 2011
-
- Lefebvre C, Manheimer E, Glanville J. Chapter 6: Searching for studies. Higgins JPT, Green S (editors). In: Cochrane Handbook for Systematic Reviews of Interventions Version 5.1.0. The Cochrane Collaboration, 2011. www.cochrane‐handbook.org, [Updated March 2011].
McKeage 2003
-
- McKeage K, Perry CM. Propofol: a review of its use in intensive care sedation of adults. CNS Drugs 2003;17(4):235‐72. [PUBMED: 12665397] - PubMed
Ozkose 2001
-
- Ozkose Z, Ercan B, Unal Y, Yardim S, Kaymaz M, Dogulu F, et al. Inhalation versus total intravenous anesthesia for lumbar disc herniation: comparison of hemodynamic effects, recovery characteristics, and cost. Journal of Neurosurgical Anesthesiology 2001;13:296‐302. [PUBMED: 11733660] - PubMed
Pinaud 1990
-
- Pinaud M, Lelausque JN, Chetanneau A, Fauchoux N, Ménégalli D, Souron R. Effects of propofol on cerebral hemodynamics and metabolism in patients with brain trauma. Anesthesiology 1990;73:404‐9. [PUBMED: 2118315] - PubMed
RevMan 5.3 [Computer program]
-
- The Nordic Cochrane Centre, The Cochrane Collaboration. Review Manager (RevMan). Version 5.3. Copenhagen: The Nordic Cochrane Centre, The Cochrane Collaboration, 2014.
Stephan 1987
-
- Stephan H, Sonntag H, Schenk HD, Kohlhausen S. Effect of Disoprivan (propofol) on the circulation and oxygen consumption of the brain and CO2 reactivity of brain vessels in the human. Anaesthesist 1987;36:60‐5. [PUBMED: 3107419] - PubMed
Visser 2001
-
- Visser K, Hassink EA, Bonsel GJ, Moen J, Kalkman CJ. Randomized controlled trial of total intravenous anesthesia with propofol versus inhalation anesthesia with isoflurane‐nitrous oxide: postoperative nausea with vomiting and economic analysis. Anesthesiology 2001;95:616‐26. [PUBMED: 11575532] - PubMed
References to other published versions of this review
Prabhakar 2017
-
- Prabhakar H, Singh GP, Mahajan C, Kapoor I, Kalaivani M, Anand V. Intravenous versus inhalational techniques for rapid emergence from anaesthesia in patients undergoing brain tumour surgery: A Cochrane systematic review. Journal of Neuroanaesthesiology and Critical Care 2017;4(1):23‐35. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous