

Micro-Computed Tomography Comparison of Preterminal Bronchioles in Centrilobular and Panlobular Emphysema
- PMID: 27611890
- PMCID: PMC5363975
- DOI: 10.1164/rccm.201602-0278OC
Micro-Computed Tomography Comparison of Preterminal Bronchioles in Centrilobular and Panlobular Emphysema
Abstract
Rationale: Very little is known about airways that are too small to be visible on thoracic multidetector computed tomography but larger than the terminal bronchioles.
Objectives: To examine the structure of preterminal bronchioles located one generation proximal to terminal bronchioles in centrilobular and panlobular emphysema.
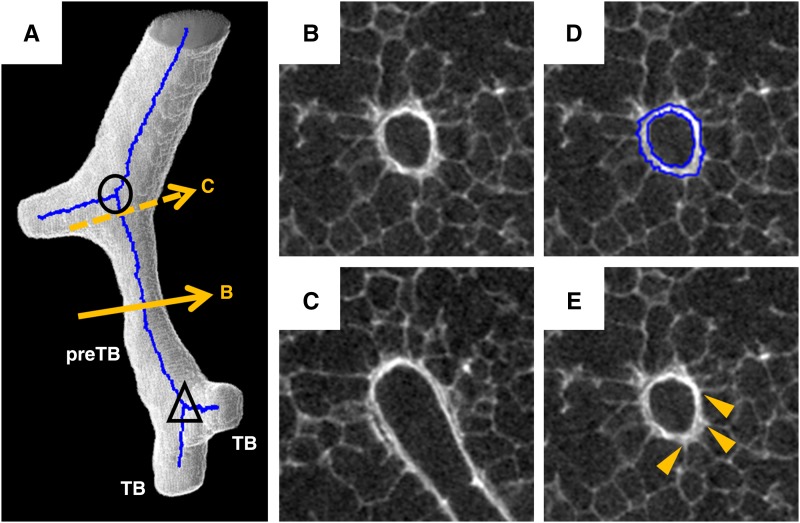
Methods: Preterminal bronchioles were identified by backtracking from the terminal bronchioles, and their centerlines were established along the entire length of their lumens. Multiple cross-sectional images perpendicular to the centerline were reconstructed to evaluate the bronchiolar wall and lumen, and the alveolar attachments to the outer airway walls in relation to emphysematous destruction in 28 lung samples from six patients with centrilobular emphysema, 20 lung samples from seven patients with panlobular emphysema associated with alpha-1 antitrypsin deficiency, and 47 samples from seven control (donor) lungs.
Measurements and main results: The preterminal bronchiolar length, wall volume, total volume (wall + lumen), lumen circularity, and number of alveolar attachments were reduced in both centrilobular and panlobular emphysema compared with control lungs. In contrast, thickening of the wall and narrowing of the lumen were more severe and heterogeneous in centrilobular than in panlobular emphysema. The bronchiolar lumen was narrower in the middle than at both ends, and the decreased number of alveolar attachments was associated with increased wall thickness in centrilobular emphysema.
Conclusions: These results provide new information about small airways pathology in centrilobular and panlobular emphysema and show that these changes affect airways that are not visible with thoracic multidetector computed tomography scans but located proximal to the terminal bronchioles in chronic obstructive pulmonary disease.
Keywords: chronic obstructive pulmonary disease; computed tomography; imaging; small airway.
Figures



Comment in
-
Multiscale Lung Imaging Provides New Insights into Disease Progression in the Chronic Obstructive Pulmonary Disease Lung.Am J Respir Crit Care Med. 2017 Mar 1;195(5):551-552. doi: 10.1164/rccm.201611-2323ED. Am J Respir Crit Care Med. 2017. PMID: 28248140 Free PMC article. No abstract available.
References
-
- Hogg JC. Pathophysiology of airflow limitation in chronic obstructive pulmonary disease. Lancet. 2004;364:709–721. - PubMed
-
- Hogg JC, Chu F, Utokaparch S, Woods R, Elliott WM, Buzatu L, Cherniack RM, Rogers RM, Sciurba FC, Coxson HO, et al. The nature of small-airway obstruction in chronic obstructive pulmonary disease. N Engl J Med. 2004;350:2645–2653. - PubMed
-
- Kim WD, Eidelman DH, Izquierdo JL, Ghezzo H, Saetta MP, Cosio MG. Centrilobular and panlobular emphysema in smokers. Two distinct morphologic and functional entities. Am Rev Respir Dis. 1991;144:1385–1390. - PubMed
-
- Saetta M, Kim WD, Izquierdo JL, Ghezzo H, Cosio MG. Extent of centrilobular and panacinar emphysema in smokers’ lungs: pathological and mechanical implications. Eur Respir J. 1994;7:664–671. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
