

Chronic Obstructive Pulmonary Disease Subtypes. Transitions over Time
- PMID: 27611911
- PMCID: PMC5017635
- DOI: 10.1371/journal.pone.0161710
Chronic Obstructive Pulmonary Disease Subtypes. Transitions over Time
Abstract
Background: Although subtypes of chronic obstructive pulmonary disease are recognized, it is unknown what happens to these subtypes over time. Our objectives were to assess the stability of cluster-based subtypes in patients with stable disease and explore changes in clusters over 1 year.
Methods: Multiple correspondence and cluster analysis were used to evaluate data collected from 543 stable patients included consecutively from 5 respiratory outpatient clinics.
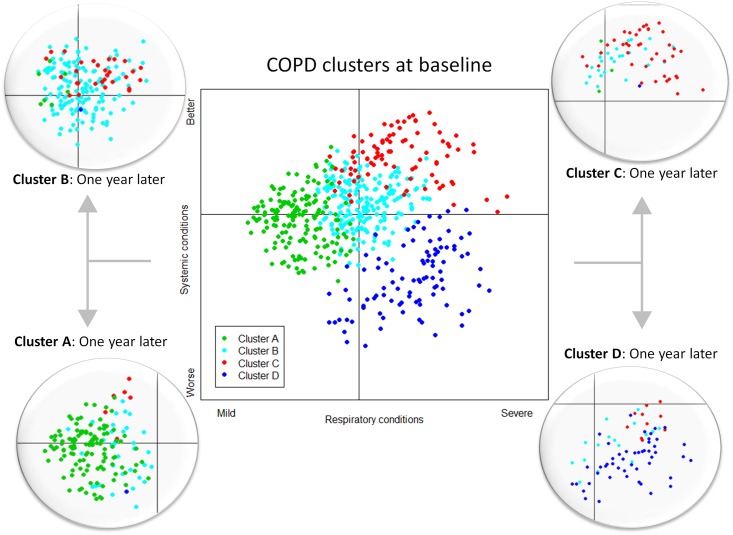
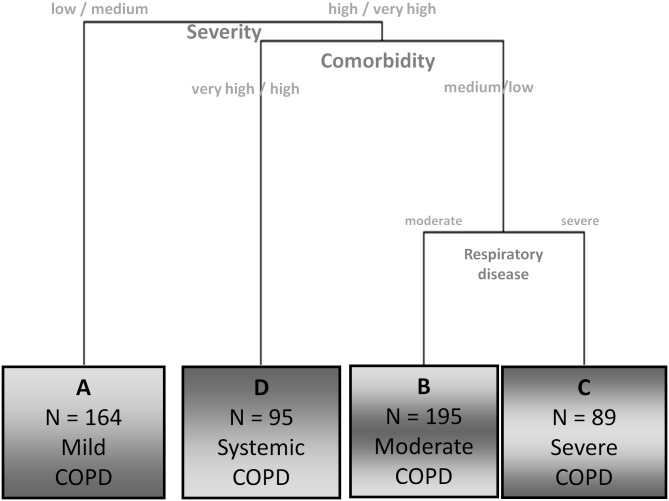
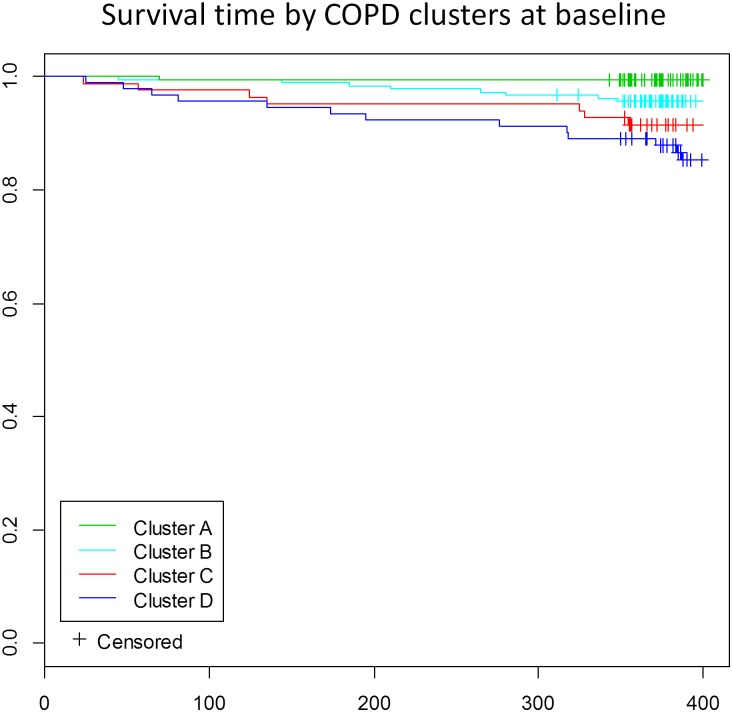
Results: Four subtypes were identified. Three of them, A, B, and C, had marked respiratory profiles with a continuum in severity of several variables, while the fourth, subtype D, had a more systemic profile with intermediate respiratory disease severity. Subtype A was associated with less dyspnea, better health-related quality of life and lower Charlson comorbidity scores, and subtype C with the most severe dyspnea, and poorer pulmonary function and quality of life, while subtype B was between subtypes A and C. Subtype D had higher rates of hospitalization the previous year, and comorbidities. After 1 year, all clusters remained stable. Generally, patients continued in the same subtype but 28% migrated to another cluster. Together with movement across clusters, patients showed changes in certain characteristics (especially exercise capacity, some variables of pulmonary function and physical activity) and changes in outcomes (quality of life, hospitalization and mortality) depending on the new cluster they belonged to.
Conclusions: Chronic obstructive pulmonary disease clusters remained stable over 1 year. Most patients stayed in their initial subtype cluster, but some moved to another subtype and accordingly had different outcomes.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Identification of five clusters of comorbidities in a longitudinal Japanese chronic obstructive pulmonary disease cohort.Respir Med. 2016 Aug;117:272-9. doi: 10.1016/j.rmed.2016.07.002. Epub 2016 Jul 7. Respir Med. 2016. PMID: 27492541
-
Relation between upper-limb muscle strength with exercise capacity, quality of life and dyspnea in patients with severe chronic obstructive pulmonary disease.Clin Respir J. 2018 Mar;12(3):1257-1263. doi: 10.1111/crj.12659. Epub 2017 Jun 22. Clin Respir J. 2018. PMID: 28618190
-
Excess Ventilation in Chronic Obstructive Pulmonary Disease-Heart Failure Overlap. Implications for Dyspnea and Exercise Intolerance.Am J Respir Crit Care Med. 2017 Nov 15;196(10):1264-1274. doi: 10.1164/rccm.201704-0675OC. Am J Respir Crit Care Med. 2017. PMID: 28665692
-
The Link between Reduced Inspiratory Capacity and Exercise Intolerance in Chronic Obstructive Pulmonary Disease.Ann Am Thorac Soc. 2017 Jul;14(Supplement_1):S30-S39. doi: 10.1513/AnnalsATS.201610-834FR. Ann Am Thorac Soc. 2017. PMID: 28398073 Review.
-
Lung hyperinflation in chronic obstructive pulmonary disease: mechanisms, clinical implications and treatment.Expert Rev Respir Med. 2014 Dec;8(6):731-49. doi: 10.1586/17476348.2014.949676. Epub 2014 Aug 27. Expert Rev Respir Med. 2014. PMID: 25159007 Review.
Cited by
-
Cost-effectiveness of home care compared to hospital care in patients with chronic obstructive pulmonary disease (COPD): a systematic review.Front Med (Lausanne). 2024 Oct 3;11:1405840. doi: 10.3389/fmed.2024.1405840. eCollection 2024. Front Med (Lausanne). 2024. PMID: 39421874 Free PMC article.
-
One-Year Evolution of Symptoms and Health Status of the COPD Multi-Dimensional Phenotypes: Results from the Follow-Up of the STORICO Observational Study.Int J Chron Obstruct Pulmon Dis. 2021 Apr 20;16:1007-1020. doi: 10.2147/COPD.S289697. eCollection 2021. Int J Chron Obstruct Pulmon Dis. 2021. PMID: 33907389 Free PMC article.
-
COPD classification models and mortality prediction capacity.Int J Chron Obstruct Pulmon Dis. 2019 Mar 7;14:605-613. doi: 10.2147/COPD.S184695. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 30880950 Free PMC article.
-
Economic Burden of Chronic Obstructive Pulmonary Disease (COPD): A Systematic Literature Review.Int J Chron Obstruct Pulmon Dis. 2020 Feb 26;15:439-460. doi: 10.2147/COPD.S234942. eCollection 2020. Int J Chron Obstruct Pulmon Dis. 2020. PMID: 32161455 Free PMC article.
-
COPD stands for complex obstructive pulmonary disease.Eur Respir Rev. 2018 Jun 6;27(148):180027. doi: 10.1183/16000617.0027-2018. Print 2018 Jun 30. Eur Respir Rev. 2018. PMID: 29875138 Free PMC article. Review.
References
-
- Dornhorst AC. Respiratory insufficiency (Frederick Price Memorial Lecture). Lancet 1955; 1: 1185–1187. - PubMed
-
- Agusti A, Calverley PM, Celli B, Coxson HO, Edwards LD, Lomas DA, et al.; Evaluation of COPD Longitudinally to Identify Predictive Surrogate Endpoints (ECLIPSE) investigators. Characterisation of COPD heterogeneity in the ECLIPSE cohort. Respir Res 2010;11:122 10.1186/1465-9921-11-122 - DOI - PMC - PubMed
-
- Celli BC, Cote CG, Marín JM, Casanova C, Montes de Oca M, Mendez RA, et al. The body-mass index, airflow obstruction, dyspnea, and exercise capacity index in chronic obstructive pulmonary disease. N Engl J Med 2004; 350: 1005–1012. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
