

Hippocampal Formation Maldevelopment and Sudden Unexpected Death across the Pediatric Age Spectrum
- PMID: 27612489
- PMCID: PMC6281079
- DOI: 10.1093/jnen/nlw075
Hippocampal Formation Maldevelopment and Sudden Unexpected Death across the Pediatric Age Spectrum
Abstract
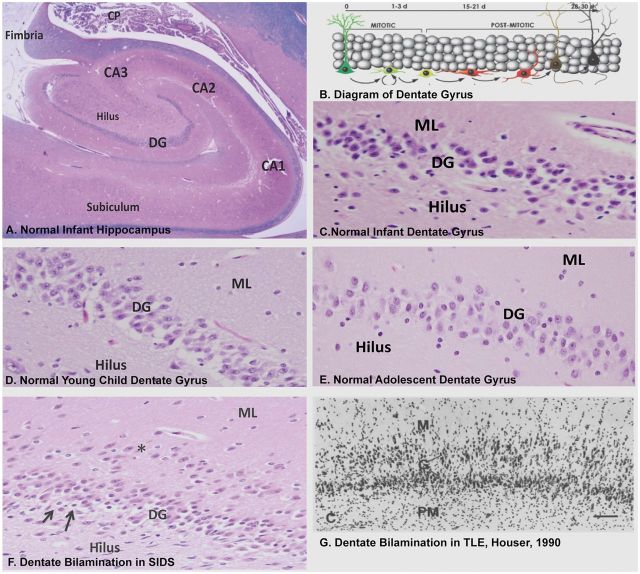
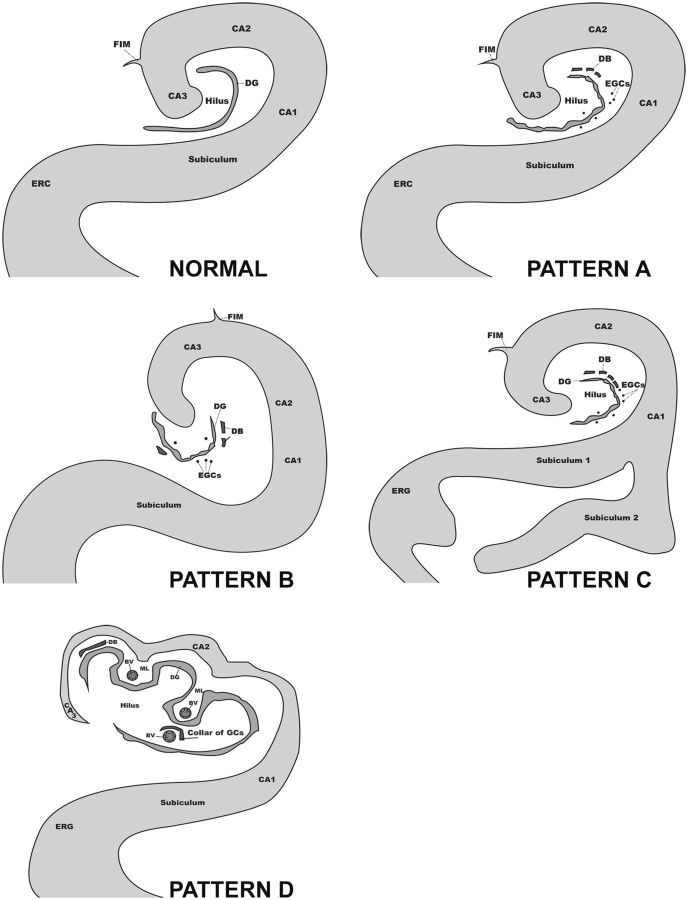
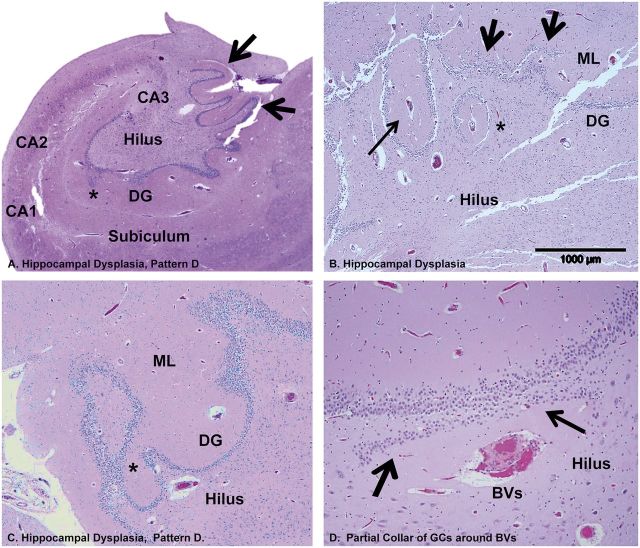
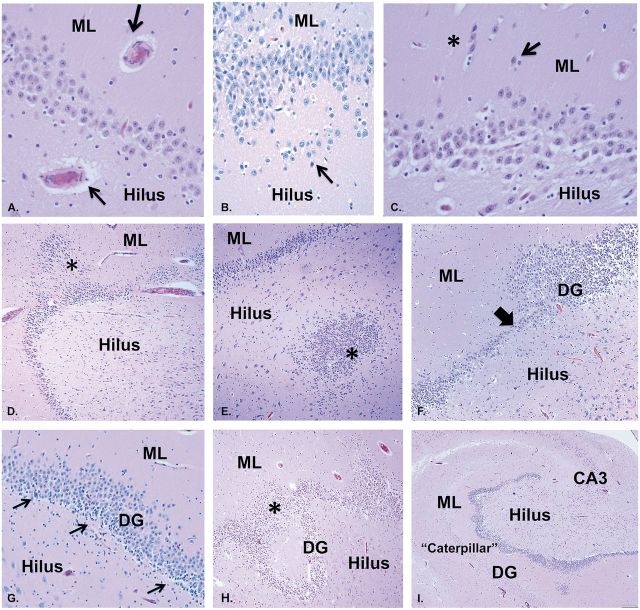
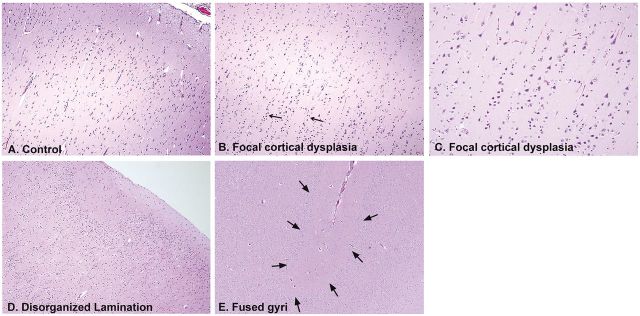
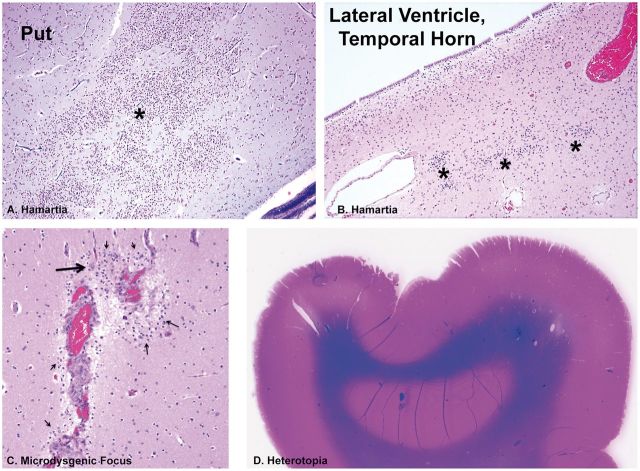
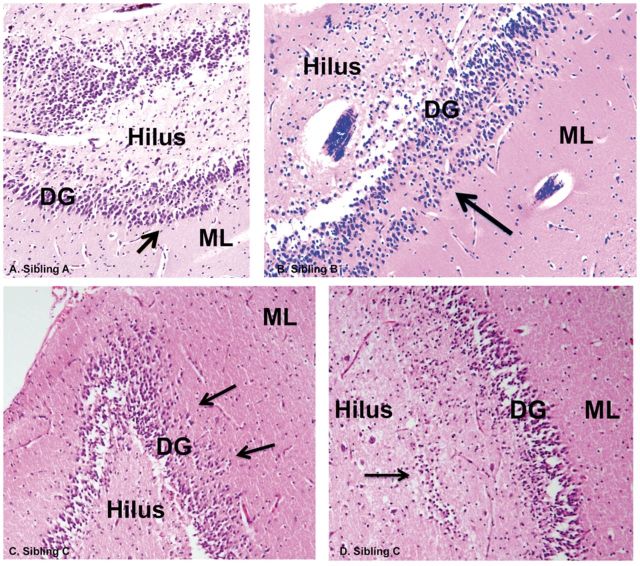
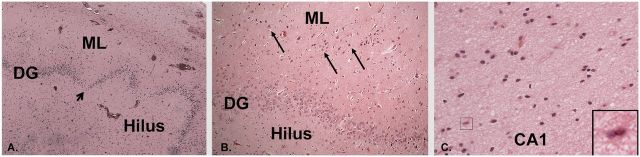
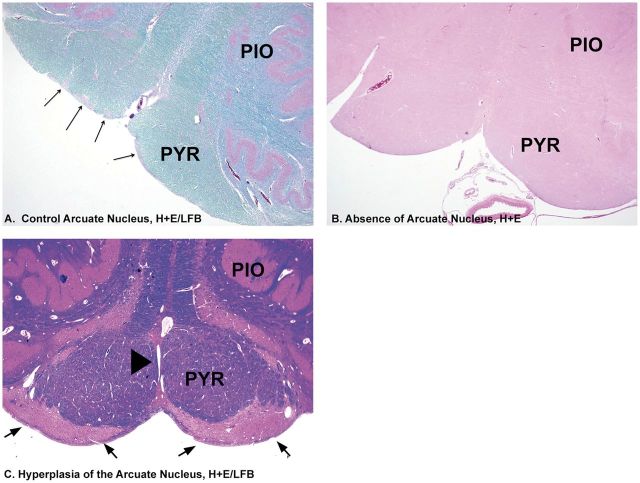
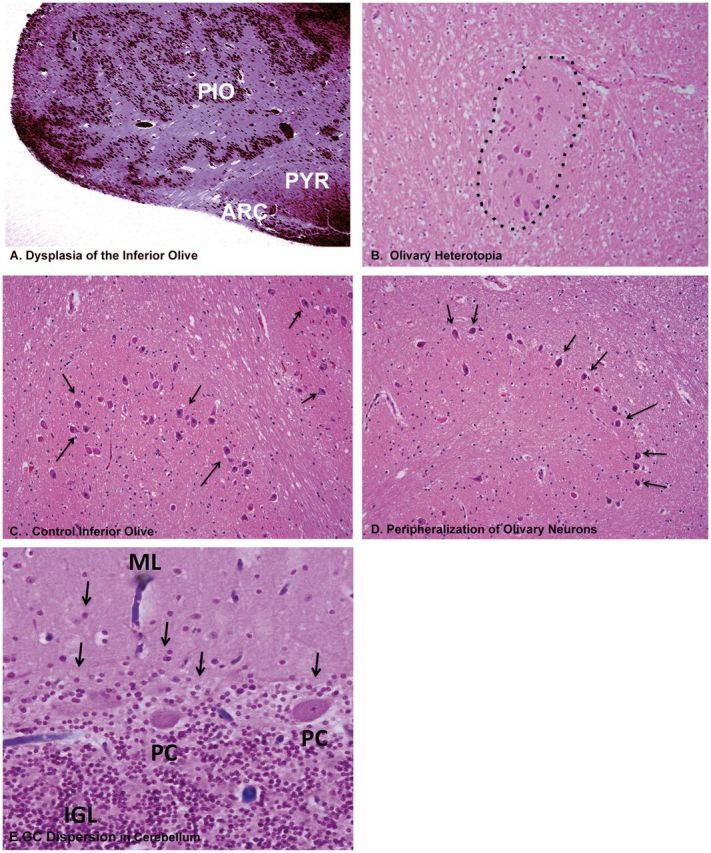
Sudden infant death syndrome (SIDS) and sudden unexplained death in childhood (SUDC) are defined as sudden death in a child remaining unexplained despite autopsy and death scene investigation. They are distinguished from each other by age criteria, i.e. with SIDS under 1 year and SUDC over 1 year. Our separate studies of SIDS and SUDC provide evidence of shared hippocampal abnormalities, specifically focal dentate bilamination, a lesion classically associated with temporal lobe epilepsy, across the 2 groups. In this study, we characterized the clinicopathologic features in a retrospective case series of 32 children with sudden death and hippocampal formation (HF) maldevelopment. The greatest frequency of deaths was between 3 weeks and 3 years (81%, 26/32). Dentate anomalies were found across the pediatric age spectrum, supporting a common vulnerability that defies the 1-year age cutoff between SIDS and SUDC. Twelve cases (38%) had seizures, including 7 only with febrile seizures. Subicular anomalies were found in cases over 1 year of age and were associated with increased risk of febrile seizures. Sudden death associated with HF maldevelopment reflects a complex interaction of intrinsic and extrinsic factors that lead to death at different pediatric ages, and may be analogous to sudden unexplained death in epilepsy.
Keywords: Dentate gyrus; Febrile seizures; Granule cell dispersion; Sudden infant death syndrome (SIDS); Sudden unexpected death in pediatrics with hippocampal formation maldevelopment (SUDP-HFM); Sudden unexplained death in childhood (SUDC); Sudden unexplained death in epilepsy (SUDEP).
© 2016 American Association of Neuropathologists, Inc. All rights reserved.
Figures
References
-
- Beckwith JB. Defining the sudden infant death syndrome . Arch Pediatr Adolesc Med 2003. ; 157 : 286 – 90 - PubMed
-
- Willinger M, James LS, Catz C. Defining the sudden infant death syndrome (SIDS): deliberations of an expert panel convened by the National Institute of Child Health and Human Development . Pediatr Pathol 1991. ; 11 : 677 – 84 - PubMed
-
- Krous HF, Chadwick AM, Crandall L , et al. . Sudden unexpected death in childhood: A report of 50 cases . Pediatr Dev Pathol 2005. ; 8 : 307 – 19 - PubMed
-
- Moon RY , Task Force on Sudden Infant Death Syndrome . SIDS and other sleep-related infant deaths: expansion of recommendations for a safe infant sleeping environment . Pediatrics 2011. ; 128 : 1030 – 9 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
