

Putting Infection Dynamics at the Heart of Chagas Disease
- PMID: 27612651
- PMCID: PMC5086431
- DOI: 10.1016/j.pt.2016.08.009
Putting Infection Dynamics at the Heart of Chagas Disease
Abstract
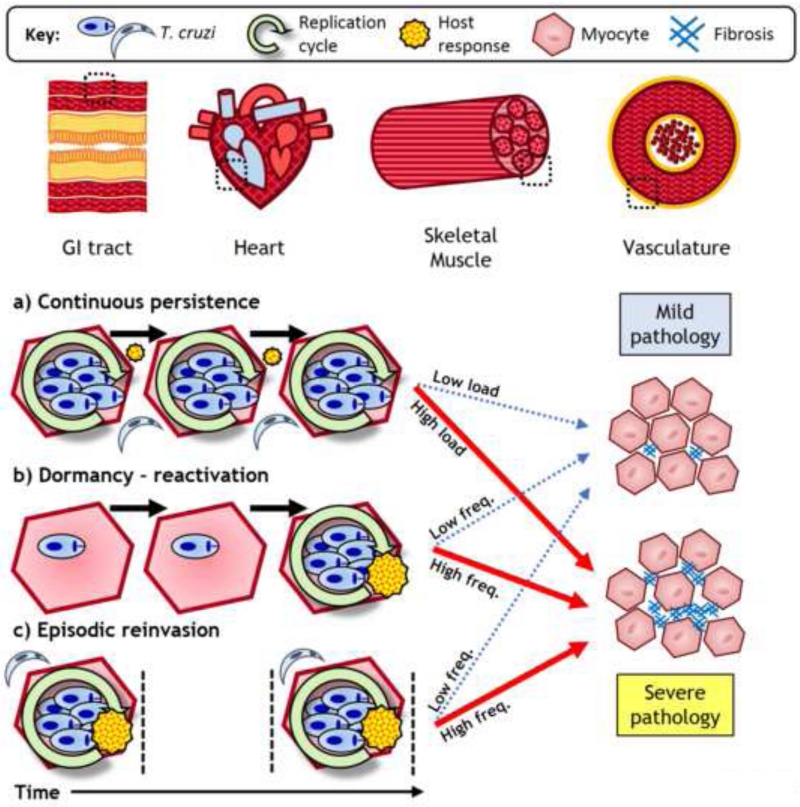
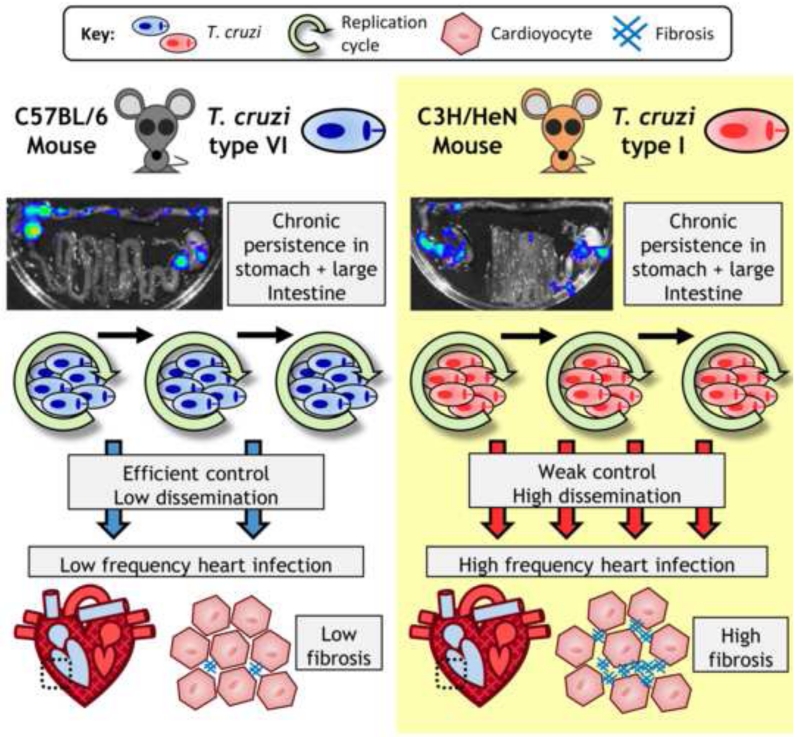
In chronic Trypanosoma cruzi infections, parasite burden is controlled by effective, but nonsterilising immune responses. Infected cells are difficult to detect because they are scarce and focally distributed in multiple sites. However, advances in detection technologies have established a link between parasite persistence and the pathogenesis of Chagas heart disease. Long-term persistence likely involves episodic reinvasion as well as continuous infection, to an extent that varies between tissues. The primary reservoir sites in humans are not definitively known, but analysis of murine models has identified the gastrointestinal tract. Here, we highlight that quantitative, spatial, and temporal aspects of T. cruzi infection are central to a fuller understanding of the association between persistence, pathogenesis, and immunity, and for optimising treatment.
Copyright © 2016 Elsevier Ltd. All rights reserved.
Figures
References
-
- Rassi A, Jr, et al. Chagas disease. Lancet. 2010;375:1388–1402. - PubMed
-
- Laranja FS, et al. Chagas’ Disease: A Clinical, Epidemiologic, and Pathologic Study. Circulation. 1956;14:1035–1060. - PubMed
-
- Barbosa A.d.A., Jr., Andrade ZA. Identificação do Trypanosoma cruzi nos tecidos extracardíacos de portadores de miocardite crônica chagásica. Revista da Sociedade Brasileira de Medicina Tropical. 1984;17:123–126.
-
- Tarleton RL. Parasite persistence in the aetiology of Chagas disease. International Journal for Parasitology. 2001;31:549–553. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
