

Autoantibody Signature Enhances the Positive Predictive Power of Computed Tomography and Nodule-Based Risk Models for Detection of Lung Cancer
- PMID: 27615397
- PMCID: PMC5367043
- DOI: 10.1016/j.jtho.2016.08.143
Autoantibody Signature Enhances the Positive Predictive Power of Computed Tomography and Nodule-Based Risk Models for Detection of Lung Cancer
Abstract
Introduction: The incidence of pulmonary nodules is increasing with the movement toward screening for lung cancer by low-dose computed tomography. Given the large number of benign nodules detected by computed tomography, an adjunctive test capable of distinguishing malignant from benign nodules would benefit practitioners. The ability of the EarlyCDT-Lung blood test (Oncimmune Ltd., Nottingham, United Kingdom) to make this distinction by measuring autoantibodies to seven tumor-associated antigens was evaluated in a prospective registry.
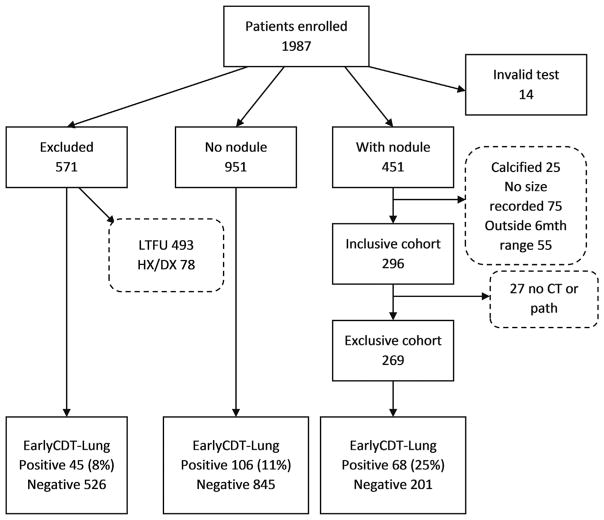
Methods: Of the members of a cohort of 1987 individuals with Health Insurance Portability and Accountability Act authorization, those with pulmonary nodules detected, imaging, and pathology reports were reviewed. All patients for whom a nodule was identified within 6 months of testing by EarlyCDT-Lung were included. The additivity of the test to nodule size and nodule-based risk models was explored.
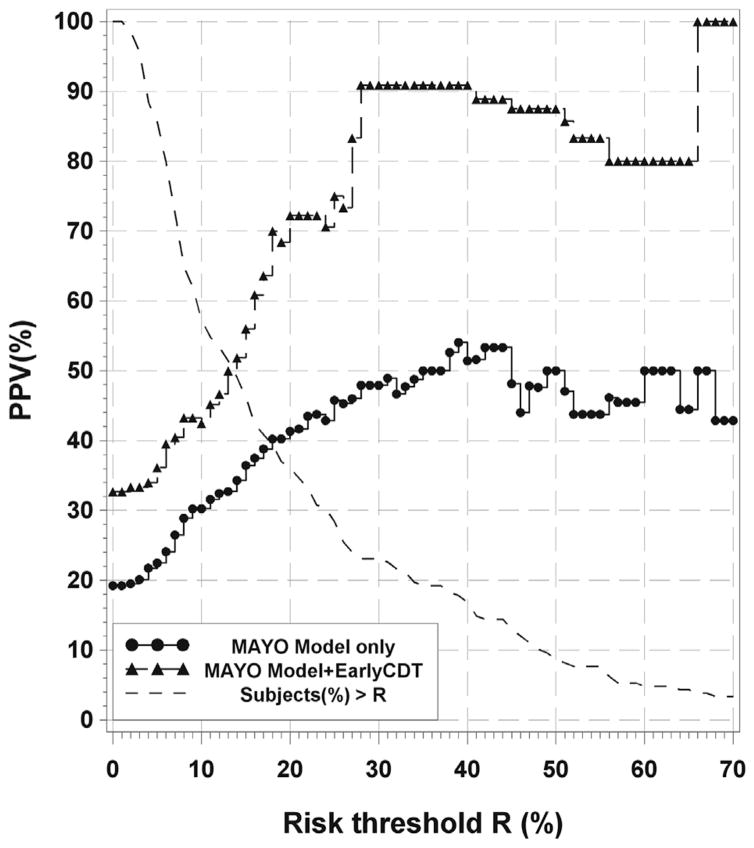
Results: A total of 451 patients (32%) had at least one nodule, leading to 296 eligible patients after exclusions, with a lung cancer prevalence of 25%. In 4- to 20-mm nodules, a positive test result represented a greater than twofold increased relative risk for development of lung cancer as compared with a negative test result. Also, when the "both-positive rule" for combining binary tests was used, adding EarlyCDT-Lung to risk models improved diagnostic performance with high specificity (>92%) and positive predictive value (>70%).
Conclusions: A positive autoantibody test result reflects a significant increased risk for malignancy in lung nodules 4 to 20 mm in largest diameter. These data confirm that EarlyCDT-Lung may add value to the armamentarium of the practitioner in assessing the risk for malignancy in indeterminate pulmonary nodules.
Keywords: Autoantibodies; CT scanning; Lung cancer; Pulmonary nodules; Risk models.
Copyright © 2016 International Association for the Study of Lung Cancer. Published by Elsevier Inc. All rights reserved.
Figures

References
-
- Gould MJ, Tang T, Liu IA, et al. Recent trends in the identification of incidental pulmonary nodules. Am J Respir Crit Care Med. 2015;192:1208–1214. - PubMed
-
- Swensen SJ, Jett JR, Hartman TE, et al. Lung cancer screening with CT: Mayo Clinic experience. Radiology. 2003;226:756–761. - PubMed
-
- Jett JR. Limitations of screening for lung cancer with low-dose spiral computed tomography. Clin Cancer Res. 2005;11:4988s–4992s. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
