

Effective Botulinum Toxin Injection Guide for Treatment of Temporal Headache
- PMID: 27618099
- PMCID: PMC5037491
- DOI: 10.3390/toxins8090265
Effective Botulinum Toxin Injection Guide for Treatment of Temporal Headache
Abstract
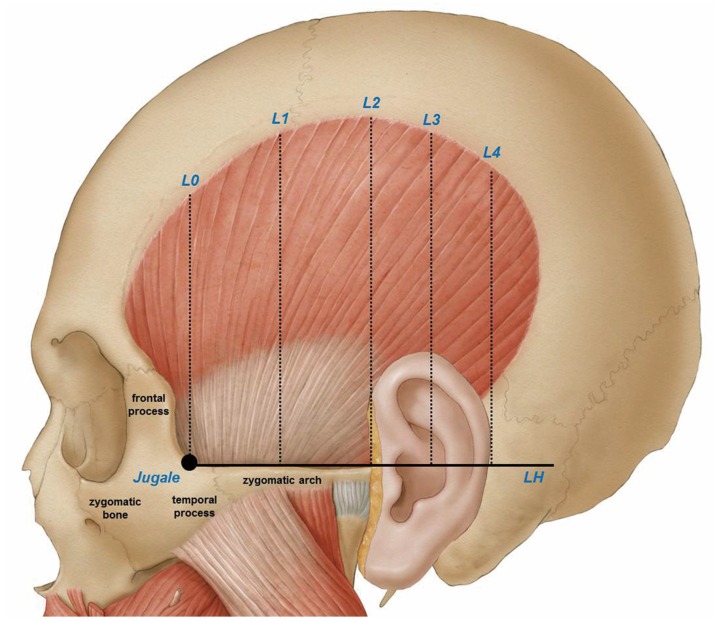
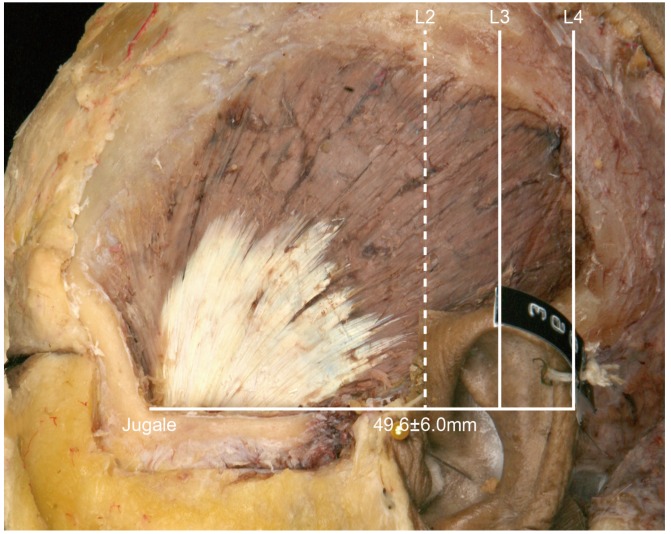
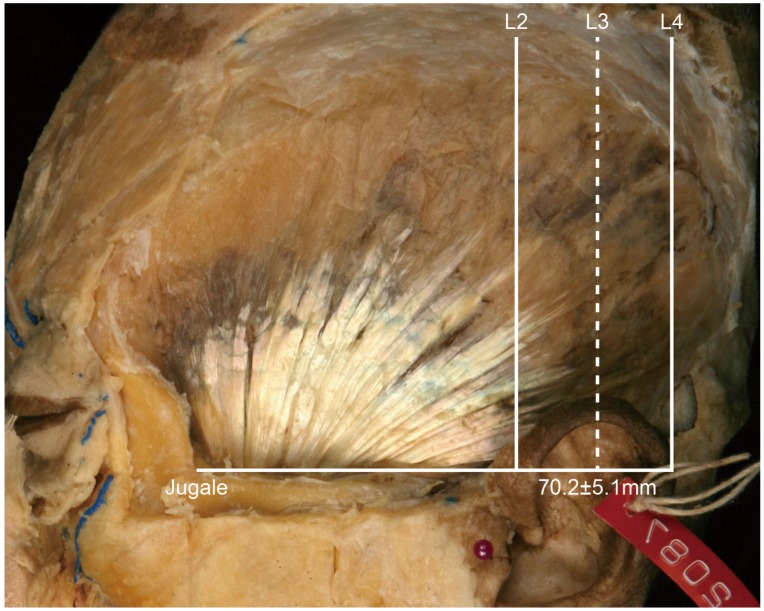
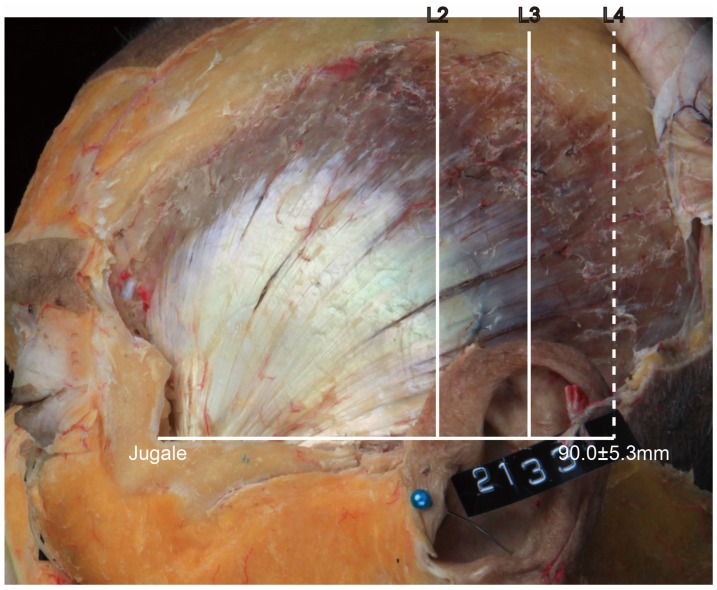
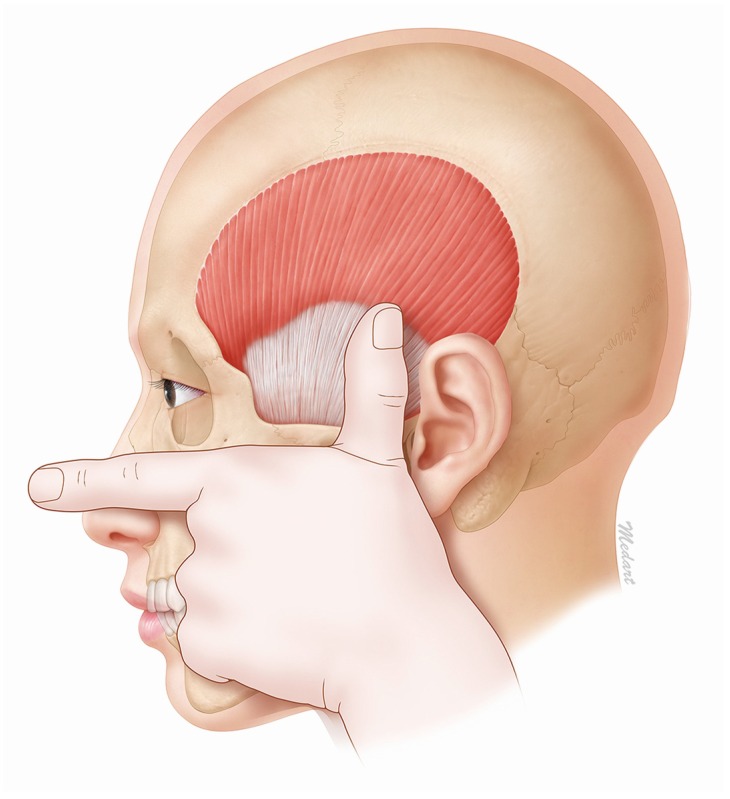
This study involved an extensive analysis of published research on the morphology of the temporalis muscle in order to provide an anatomical guideline on how to distinguish the temporalis muscle and temporalis tendon by observing the surface of the patient's face. Twenty-one hemifaces of cadavers were used in this study. The temporalis muscles were dissected clearly for morphological analysis between the temporalis muscle and tendon. The posterior border of the temporalis tendon was classified into three types: in Type I the posterior border of the temporalis tendon is located in front of reference line L2 (4.8%, 1/21), in Type II it is located between reference lines L2 and L3 (85.7%, 18/21), and in Type III it is located between reference lines L3 and L4 (9.5%, 2/21). The vertical distances between the horizontal line passing through the jugale (LH) and the temporalis tendon along each of reference lines L0, L1, L2, L3, and L4 were 29.7 ± 6.8 mm, 45.0 ± 8.8 mm, 37.7 ± 11.1 mm, 42.5 ± 7.5 mm, and 32.1 ± 0.4 mm, respectively. BoNT-A should be injected into the temporalis muscle at least 45 mm vertically above the zygomatic arch. This will ensure that the muscle region is targeted and so produce the greatest clinical effect with the minimum concentration of BoNT-A.
Keywords: Sihler staining; botulinum toxin type A; injection site; migraine; temporalis muscle.
Conflict of interest statement
The authors declare no conflict of interest.
Figures

References
-
- Carruthers J., Carruthers A. Botulinum toxin (Botox) chemodenervation for facial rejuvenation. Facial Plast Surg. Clin. North Am. 2001;9:197–204. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
