

Gender Differences in Appropriate Shocks and Mortality among Patients with Primary Prophylactic Implantable Cardioverter-Defibrillators: Systematic Review and Meta-Analysis
- PMID: 27618617
- PMCID: PMC5019464
- DOI: 10.1371/journal.pone.0162756
Gender Differences in Appropriate Shocks and Mortality among Patients with Primary Prophylactic Implantable Cardioverter-Defibrillators: Systematic Review and Meta-Analysis
Abstract
Background: Some but not all prior studies have shown that women receiving a primary prophylactic implantable cardioverter defibrillator (ICD) have a lower risk of death and appropriate shocks than men.
Purpose: To evaluate the effect of gender on the risk of appropriate shock, all-cause mortality and inappropriate shock in contemporary studies of patients receiving a primary prophylactic ICD.
Data source: PubMed, LIVIVO, Cochrane CENTRAL between 2010 and 2016.
Study selection: Studies providing at least 1 gender-specific risk estimate for the outcomes of interest.
Data extraction: Abstracts were screened independently for potentially eligible studies for inclusion. Thereby each abstract was reviewed by at least two authors.
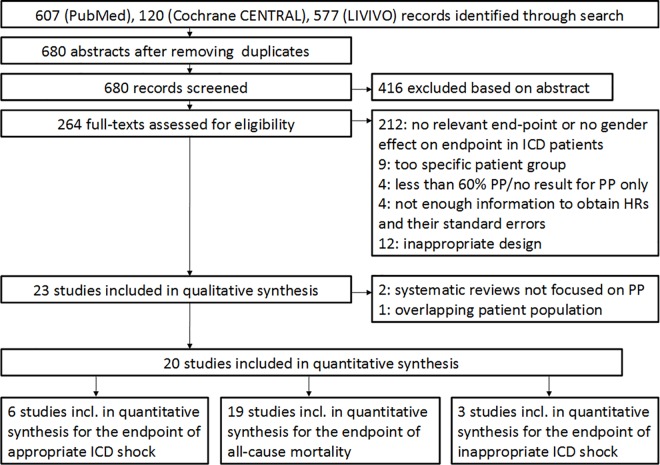
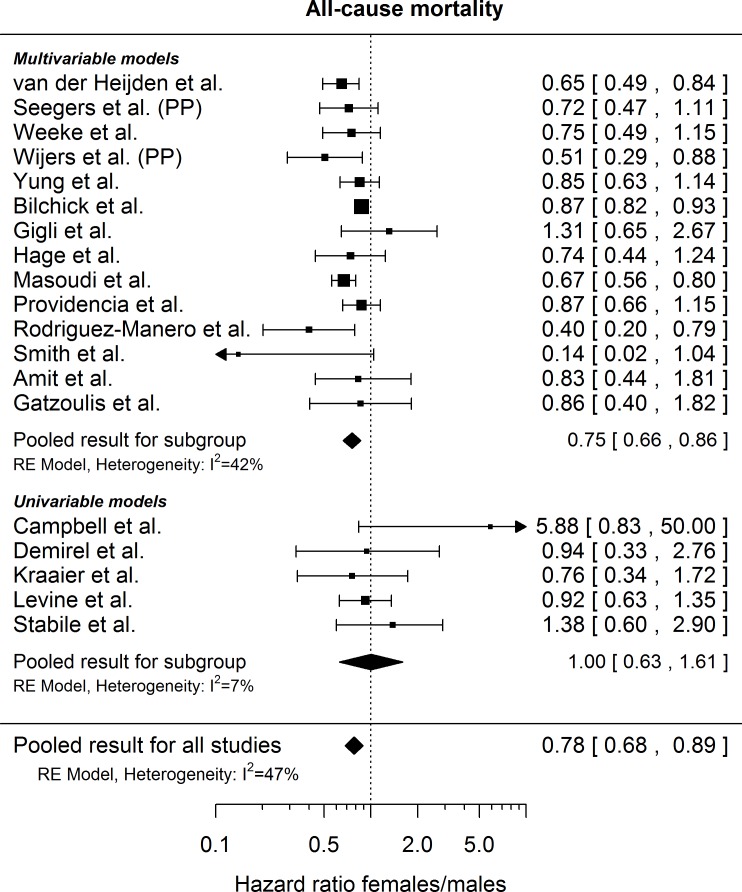
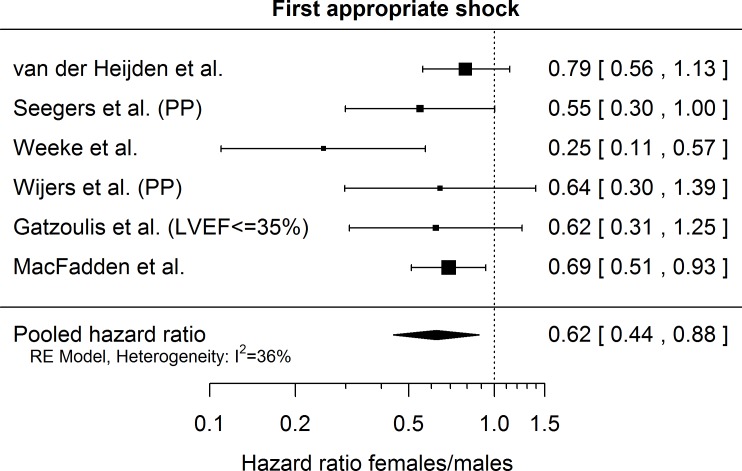
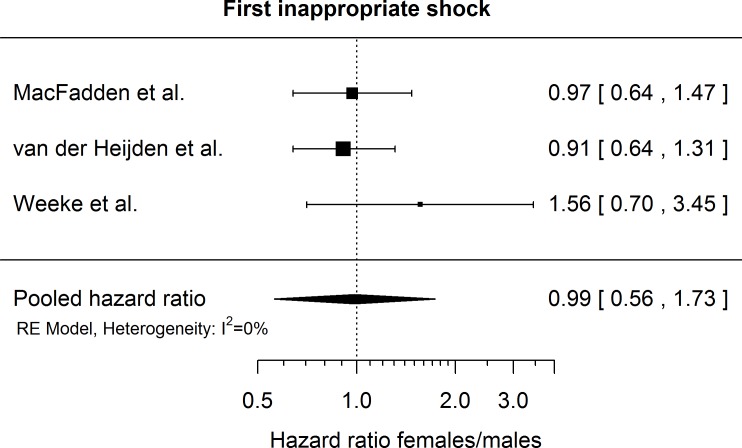
Data synthesis: Out of 680 abstracts retained by our search strategy, 20 studies including 46'657 patients had gender-specific information on at least one of the relevant endpoints. Mean age across the individual studies varied between 58 and 69 years. The proportion of women enrolled ranged from 10% to 30%. Across 6 available studies, women had a significantly lower risk of first appropriate shock compared with men (pooled multivariable adjusted hazard ratio 0.62 (95% CI [0.44; 0.88]). Across 14 studies reporting multivariable adjusted gender-specific hazard ratio estimates for all-cause mortality, women had a lower risk of death than men (pooled hazard ratio 0.75 (95% CI [0.66; 0.86]). There was no statistically significant difference for the incidence of first inappropriate shocks (3 studies, pooled hazard ratio 0.99 (95% CI [0.56; 1.73]).
Limitations: Individual patient data were not available for most studies.
Conclusion: In this large contemporary meta-analysis, women had a significantly lower risk of appropriate shocks and death than men, but a similar risk of inappropriate shocks. These data may help to select patients who benefit from primary prophylactic ICD implantation.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Al-Khatib SM, Anstrom KJ, Eisenstein EL, Peterson ED, Jollis JG, Mark DB, et al. Clinical and economic implications of the Multicenter Automatic Defibrillator Implantation Trial-II. Annals of internal medicine. 2005;142(8):593–600. . - PubMed
-
- Mark DB, Nelson CL, Anstrom KJ, Al-Khatib SM, Tsiatis AA, Cowper PA, et al. Cost-effectiveness of defibrillator therapy or amiodarone in chronic stable heart failure: results from the Sudden Cardiac Death in Heart Failure Trial (SCD-HeFT). Circulation. 2006;114(2):135–42. 10.1161/CIRCULATIONAHA.105.581884 . - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
