

Prevalence of medication discrepancies in patients with cirrhosis: a pilot study
- PMID: 27618841
- PMCID: PMC5020443
- DOI: 10.1186/s12876-016-0530-4
Prevalence of medication discrepancies in patients with cirrhosis: a pilot study
Abstract
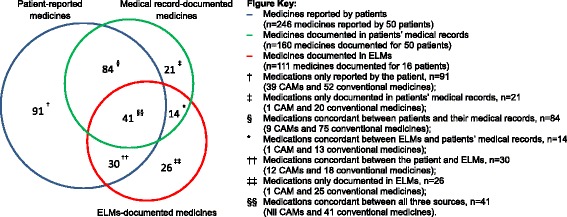
Background: Cirrhosis patients are prescribed multiple medications for their liver disease and comorbidities. Discrepancies between medicines consumed by patients and those documented in the medical record may contribute to patient harm and impair disease management. The aim of the present study was to assess the magnitude and types of discrepancies among patient-reported and medical record-documented medications in patients with cirrhosis, and examine factors associated with such discrepancies.
Methods: Fifty patients who attended a hospital hepatology outpatient clinic were interviewed using a questionnaire composed of mixed short-response and multiple-choice questions. Patients' reported medication use was compared with documentation in the hospital medical records and pharmacy database. Medication adherence was assessed using the 8-question ©Morisky Medication Adherence Scale (MMAS-8). The multivariate logistic regression model was constructed using clinically relevant and/or statistically significant variables as determined by univariate analysis. All p-values were 2-sided (α = 0.05).
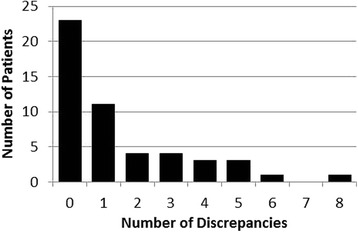
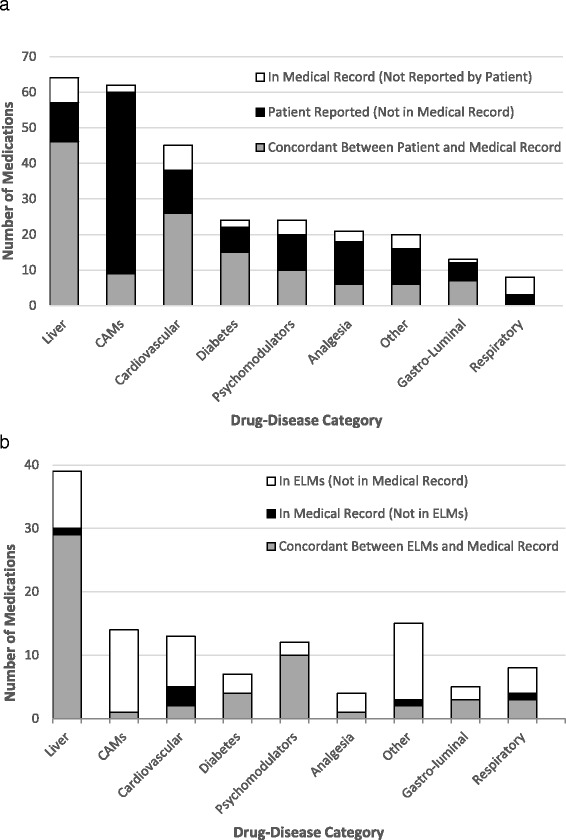
Results: Twenty-seven patients (54.0 %) had ≥1 discrepancy between reported and documented medicines. Patients with ≥1 discrepancy were older (p = 0.04) and multivariate analysis identified taking ≥5 conventional medicines or having a 'low' or 'medium' adherence ranking as independent predictors of discrepancy (adjusted OR 11.0 (95 % CI 1.8-67.4), 20.7 (95 % CI 1.3-337.7) and 49.0 (95 % CI 3.3-718.5) respectively). Concordance was highest for liver disease medicines (71.9 %) and lowest for complementary and alternative medicines (14.5 %) and respiratory medicines (0 %).
Conclusion: There is significant discrepancy between sources of patient medication information within the hepatology clinic. Medication reconciliation and medicines-management intervention may address the complex relationship between medication discrepancies, number of medications and patient adherence identified in this study.
Keywords: Ambulatory care; Complementary therapies; Liver cirrhosis; Medication adherence; Medication reconciliation.
Figures
References
-
- Deloitte Access Economics . The economic cost and health burden of liver diseases in Australia. Kingston: The Gastroenterological Society of Australia/Australian Liver Association; 2013.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
