

Cardiovascular Consequences of Childhood Secondhand Tobacco Smoke Exposure: Prevailing Evidence, Burden, and Racial and Socioeconomic Disparities: A Scientific Statement From the American Heart Association
- PMID: 27619923
- PMCID: PMC5207215
- DOI: 10.1161/CIR.0000000000000443
Cardiovascular Consequences of Childhood Secondhand Tobacco Smoke Exposure: Prevailing Evidence, Burden, and Racial and Socioeconomic Disparities: A Scientific Statement From the American Heart Association
Erratum in
-
Correction to: Cardiovascular Consequences of Childhood Secondhand Tobacco Smoke Exposure: Prevailing Evidence, Burden, and Racial and Socioeconomic Disparities: A Scientific Statement From the American Heart Association.Circulation. 2016 Oct 18;134(16):e366. doi: 10.1161/CIR.0000000000000465. Circulation. 2016. PMID: 27754954 No abstract available.
Abstract
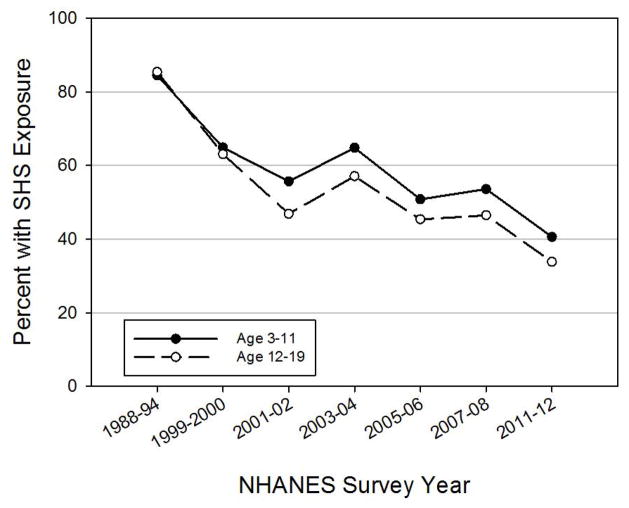
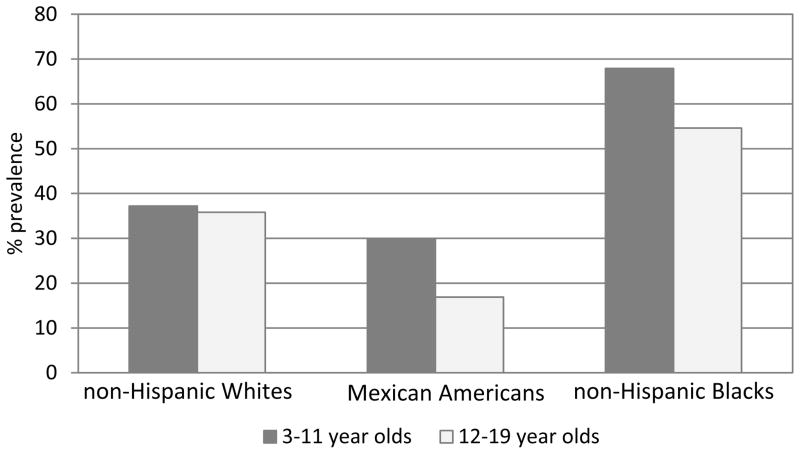
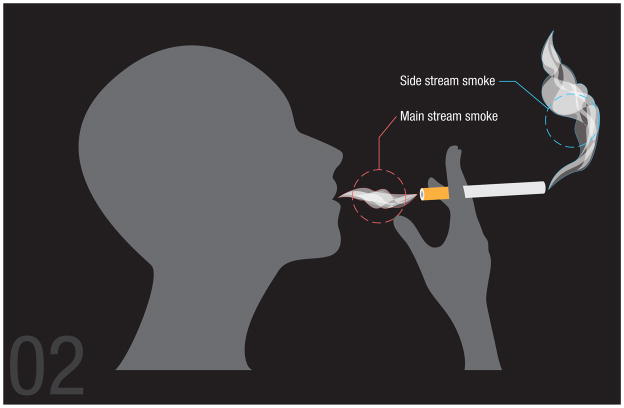
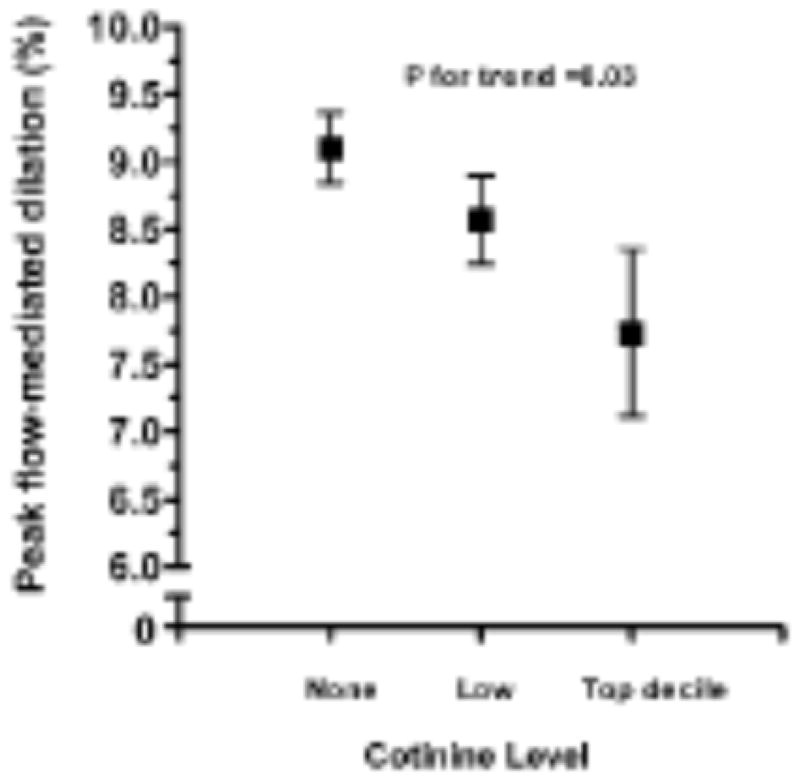
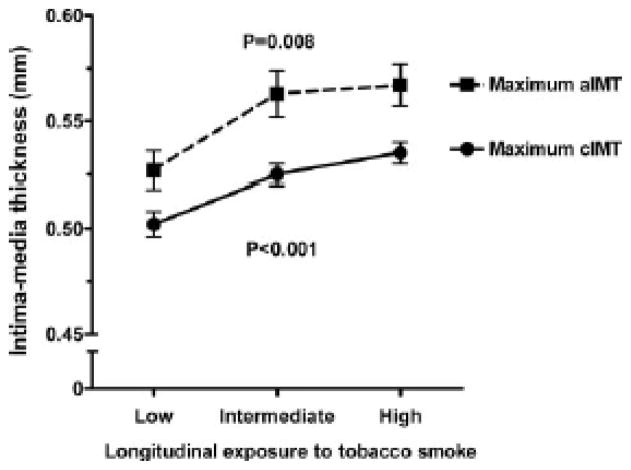
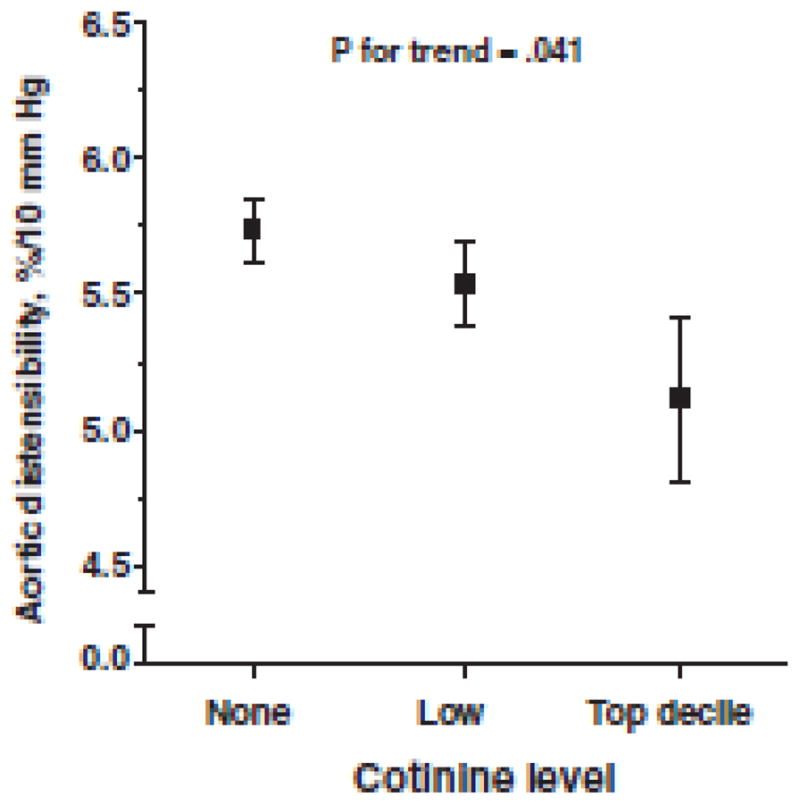
Background: Although public health programs have led to a substantial decrease in the prevalence of tobacco smoking, the adverse health effects of tobacco smoke exposure are by no means a thing of the past. In the United States, 4 of 10 school-aged children and 1 of 3 adolescents are involuntarily exposed to secondhand tobacco smoke (SHS), with children of minority ethnic backgrounds and those living in low-socioeconomic-status households being disproportionately affected (68% and 43%, respectively). Children are particularly vulnerable, with little control over home and social environment, and lack the understanding, agency, and ability to avoid SHS exposure on their own volition; they also have physiological or behavioral characteristics that render them especially susceptible to effects of SHS. Side-stream smoke (the smoke emanating from the burning end of the cigarette), a major component of SHS, contains a higher concentration of some toxins than mainstream smoke (inhaled by the smoker directly), making SHS potentially as dangerous as or even more dangerous than direct smoking. Compelling animal and human evidence shows that SHS exposure during childhood is detrimental to arterial function and structure, resulting in premature atherosclerosis and its cardiovascular consequences. Childhood SHS exposure is also related to impaired cardiac autonomic function and changes in heart rate variability. In addition, childhood SHS exposure is associated with clustering of cardiometabolic risk factors such as obesity, dyslipidemia, and insulin resistance. Individualized interventions to reduce childhood exposure to SHS are shown to be at least modestly effective, as are broader-based policy initiatives such as community smoking bans and increased taxation.
Purpose: The purpose of this statement is to summarize the available evidence on the cardiovascular health consequences of childhood SHS exposure; this will support ongoing efforts to further reduce and eliminate SHS exposure in this vulnerable population. This statement reviews relevant data from epidemiological studies, laboratory-based experiments, and controlled behavioral trials concerning SHS and cardiovascular disease risk in children. Information on the effects of SHS exposure on the cardiovascular system in animal and pediatric studies, including vascular disruption and platelet activation, oxidation and inflammation, endothelial dysfunction, increased vascular stiffness, changes in vascular structure, and autonomic dysfunction, is examined.
Conclusions: The epidemiological, observational, and experimental evidence accumulated to date demonstrates the detrimental cardiovascular consequences of SHS exposure in children.
Implications: Increased awareness of the adverse, lifetime cardiovascular consequences of childhood SHS may facilitate the development of innovative individual, family-centered, and community health interventions to reduce and ideally eliminate SHS exposure in the vulnerable pediatric population. This evidence calls for a robust public health policy that embraces zero tolerance of childhood SHS exposure.
Keywords: AHA Scientific Statement; atherosclerosis; blood vessels; child; tobacco smoke pollution.
© 2016 American Heart Association, Inc.
Figures

References
-
- US Public Health Service. Smoking and health: A report of the surgeon general (dhew publication no.(phs) 79-50066) Washington, DC: US Department of Health, Education, and Welfare; 1979.
-
- Centers for Disease Control Prevention. Vital signs: Current cigarette smoking among adults aged≥ 18 years--united states, 2005–2010. MMWR. Morbidity and mortality weekly report. 2011;60:1207. - PubMed
-
- Centers for Disease Control and Prevention. Smoking-attributable mortality, years of potential life lost, and productivity losses--united states, 2000–2004. MMWR. Morbidity and mortality weekly report. 2008;57:1226–1228. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
