

Diagnostic Accuracy of Fecal Calprotectin for Pediatric Inflammatory Bowel Disease in Primary Care: A Prospective Cohort Study
- PMID: 27621160
- PMCID: PMC5394359
- DOI: 10.1370/afm.1949
Diagnostic Accuracy of Fecal Calprotectin for Pediatric Inflammatory Bowel Disease in Primary Care: A Prospective Cohort Study
Abstract
Purpose: In specialist care, fecal calprotectin (FCal) is a commonly used noninvasive diagnostic test for ruling out inflammatory bowel disease (IBD) in children with chronic gastrointestinal symptoms. The aim of this study was to evaluate the diagnostic accuracy of FCal for IBD in symptomatic children in primary care.
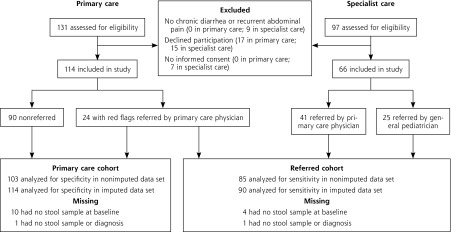
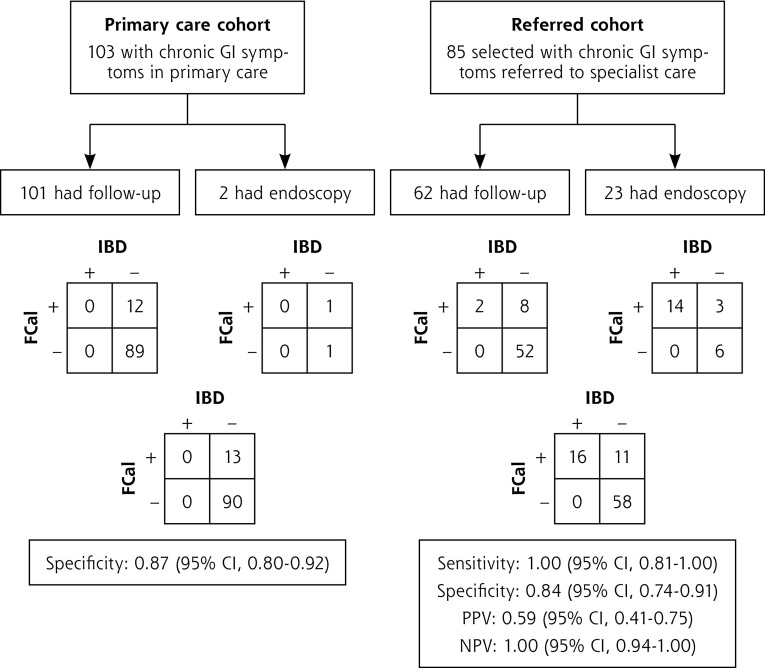
Methods: We studied 2 prospective cohorts of children with chronic diarrhea, recurrent abdominal pain, or both: children initially seen in primary care (primary care cohort) and children referred to specialist care (referred cohort). FCal (index test) was measured at baseline and compared with 1 of the 2 reference standards for IBD: endoscopic assessment or 1-year follow-up. Physicians were blinded to FCal results, and values greater than 50 μg/g feces were considered positive. We determined specificity in the primary care cohort and sensitivity in the referred cohort.
Results: None of the 114 children in the primary care cohort ultimately received a diagnosis of IBD. The specificity of FCal in the primary care cohort was 0.87 (95% CI, 0.80-0.92). Among the 90 children in the referred cohort, 17 (19%) ultimately received a diagnosis of IBD. The sensitivity of FCal in the referred cohort was 0.99 (95% CI, 0.81-1.00).
Conclusions: The findings of this study suggest that a positive FCal result in children with chronic gastrointestinal symptoms seen in primary care is not likely to be indicative of IBD. A negative FCal result is likely to be a true negative, which safely rules out IBD in children in whom a primary care physician considers referral to specialist care.
Keywords: calprotectin; child; inflammatory bowel disease; practice-based research; primary health care; sensitivity and specificity.
© 2016 Annals of Family Medicine, Inc.
Figures
References
-
- BEACH Program, AIHW General Practice Statistics and Classification Unit. Presentations of abdominal pain in Australian general practice. Aust Fam Physician. 2004;33(12):968–969. - PubMed
-
- Starfield B, Hoekelman RA, McCormick M, et al. Who provides health care to children and adolescents in the United States? Pediatrics. 1984;74(6):991–997. - PubMed
-
- Spray C, Debelle GD, Murphy MS. Current diagnosis, management and morbidity in paediatric inflammatory bowel disease. Acta Paediatr. 2001;90(4):400–405. - PubMed
-
- Kim SC, Ferry GD. Inflammatory bowel diseases in pediatric and adolescent patients: clinical, therapeutic, and psychosocial considerations. Gastroenterology. 2004;126(6):1550–1560. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources