

Pancreatic cancer: Open or minimally invasive surgery?
- PMID: 27621576
- PMCID: PMC4997638
- DOI: 10.3748/wjg.v22.i32.7301
Pancreatic cancer: Open or minimally invasive surgery?
Abstract
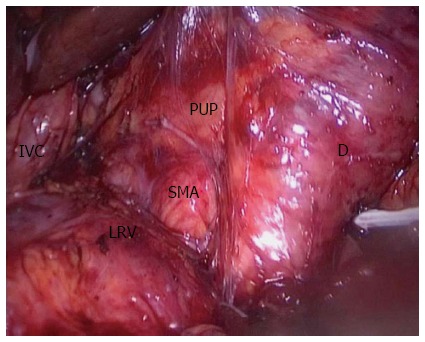
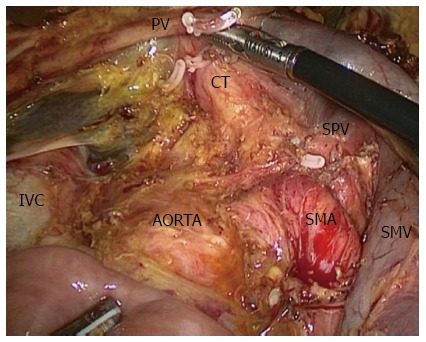
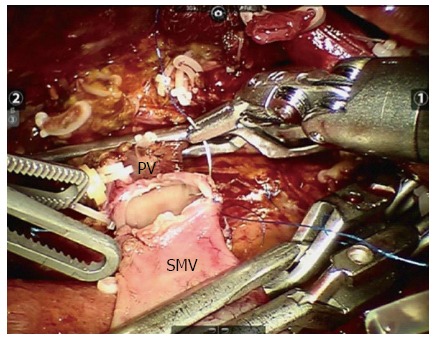
Pancreatic duct adenocarcinoma is one of the most fatal malignancies, with R0 resection remaining the most important part of treatment of this malignancy. However, pancreatectomy is believed to be one of the most challenging procedures and R0 resection remains the only chance for patients with pancreatic cancer to have a good prognosis. Some surgeons have tried minimally invasive pancreatic surgery, but the short- and long-term outcomes of pancreatic malignancy remain controversial between open and minimally invasive procedures. We collected comparative data about minimally invasive and open pancreatic surgery. The available evidence suggests that minimally invasive pancreaticoduodenectomy (MIPD) is as safe and feasible as open PD (OPD), and shows some benefit, such as less intraoperative blood loss and shorter postoperative hospital stay. Despite the limited evidence for MIPD in pancreatic cancer, most of the available data show that the short-term oncological adequacy is similar between MIPD and OPD. Some surgical techniques, including superior mesenteric artery-first approach and laparoscopic pancreatoduodenectomy with major vein resection, are believed to improve the rate of R0 resection. Laparoscopic distal pancreatectomy is less technically demanding and is accepted in more pancreatic centers. It is technically safe and feasible and has similar short-term oncological prognosis compared with open distal pancreatectomy.
Keywords: Distal pancreatectomy; Laparoscopic; Minimally invasive; Pancreatic cancer; Pancreaticoduodenectomy; Robotic.
Figures
References
-
- Siegel RL, Miller KD, Jemal A. Cancer statistics, 2016. CA Cancer J Clin. 2016;66:7–30. - PubMed
-
- Gao JJ, Song PP, Tamura S, Hasegawa K, Sugawara Y, Kokudo N, Uchida K, Orii R, Qi FH, Dong JH, et al. Standardization of perioperative management on hepato-biliary-pancreatic surgery. Drug Discov Ther. 2012;6:108–111. - PubMed
-
- Hidalgo M. Pancreatic cancer. N Engl J Med. 2010;362:1605–1617. - PubMed
-
- Shimoda M. Upon completing the 7th Sino-Japanese Symposium on Hepato-Pancreato-Biliary Disease. Biosci Trends. 2008;2:96. - PubMed
-
- Yamashita S, Sakamoto Y, Kaneko J, Tamura S, Aoki T, Sugawara Y, Hasegawa K, Kokudo N. Resection of the second portion of the duodenum sacrificing the minor papilla but preserving the pancreas for a recurrent duodenal adenocarcinoma: report of a case. Biosci Trends. 2012;6:44–47. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
