

Intra-cheek immunization as a novel vaccination route for therapeutic vaccines of head and neck squamous cell carcinomas using plasmo virus-like particles
- PMID: 27622018
- PMCID: PMC5006902
- DOI: 10.1080/2162402X.2016.1164363
Intra-cheek immunization as a novel vaccination route for therapeutic vaccines of head and neck squamous cell carcinomas using plasmo virus-like particles
Abstract
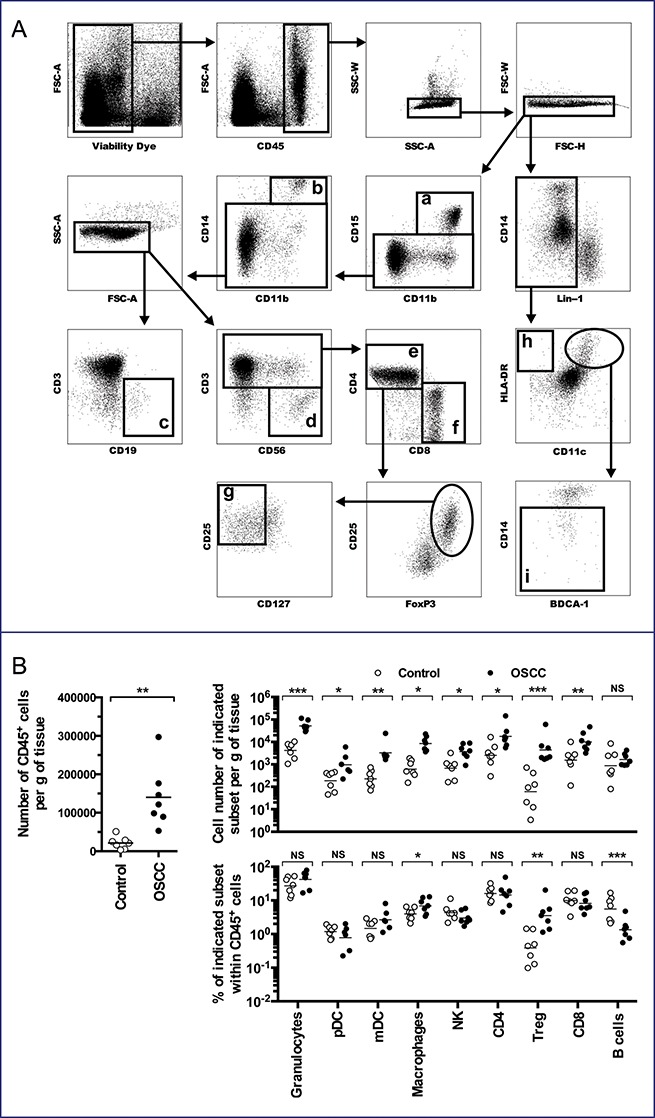
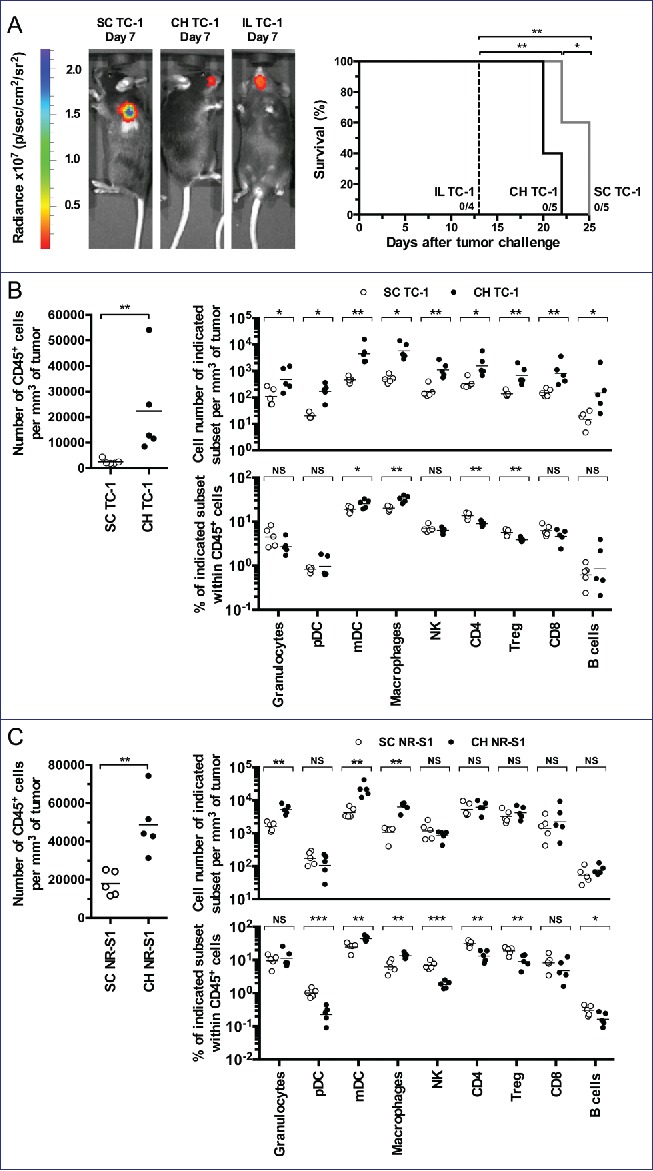
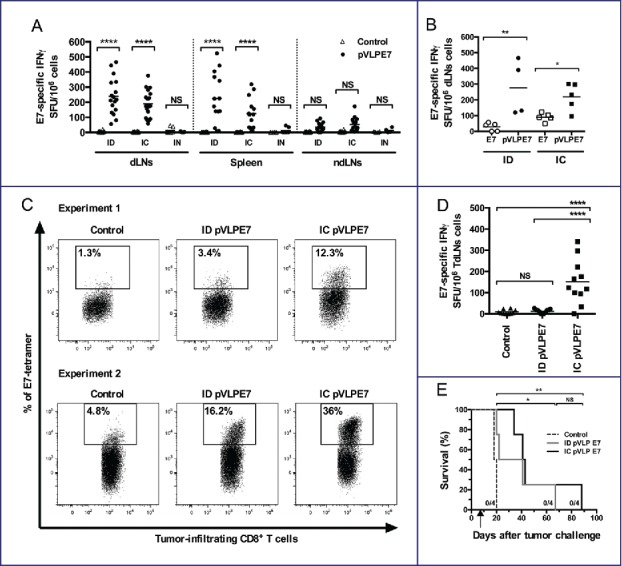
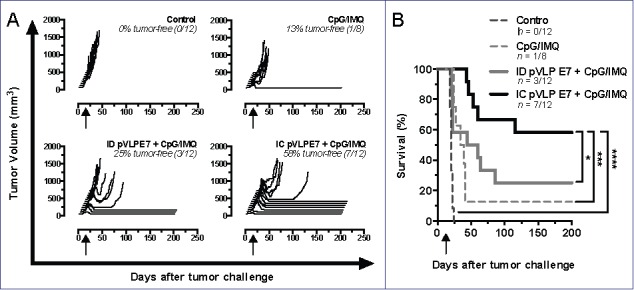
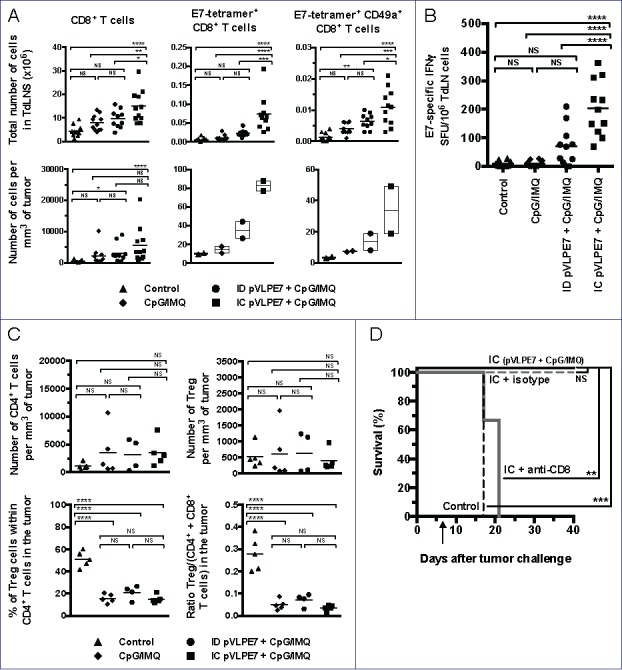
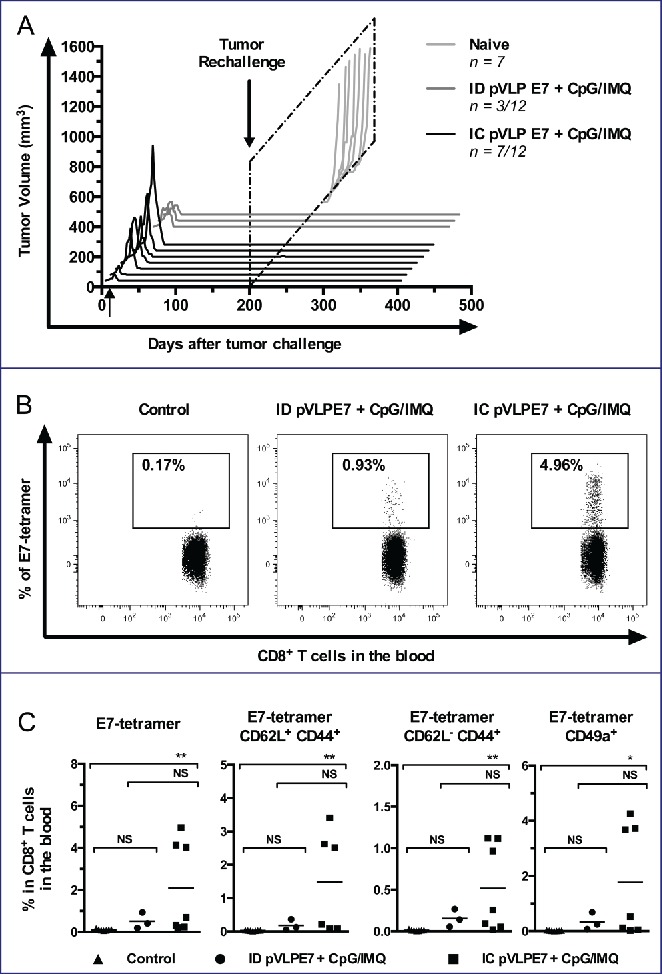
Despite current therapy, head and neck squamous cell carcinomas (HNSCCs) arising from various mucosal sites of the upper aero-digestive tract frequently relapse in a loco-regional manner and have a poor prognosis. Our objective was to validate an innovative mucosal route of vaccination using plasmo virus-like particles (pVLPs) in a pre-clinical orthotopic model of HNSCCs. For this purpose, we used pVLP-E7, that are plasmid DNA encoding retroviral virus-like particles carrying a truncated E7 oncoprotein from HPV-16 as antigen model, to vaccinate mice bearing pre-established TC-1 tumors implanted into the buccal mucosa. pVLP-E7 were combined with clinical grade TLR agonists (Imiquimod and CpG-ODN). In this pre-clinical orthotopic model, whose tumor microenvironment resembles to those of human HNSCCs, different mucosal vaccination routes were tested for their ability to elicit efficient immune and antitumoral responses. Results showed that mucosal intra-cheek (IC) vaccinations using pVLP-E7, comparatively to intradermic vaccinations (ID), gave rise to higher mobilization of mucosal (CD49a(+)) CD8(+) specific effector T cells in both tumor draining lymph nodes (TdLNs) and tumor microenvironment resulting in better antitumor effects and in a long-term protection against tumor rechallenge. In vivo CD8(+) depletion demonstrated that antitumoral effects were fully dependent upon the presence of CD8(+) T cells. Validation of IC mucosal vaccinations with pVLPs combined with adjuvants using a pre-clinical orthotopic model of HNSCC provides valuable pre-clinical data to rapidly envision the use of such therapeutic vaccines in patients with HNSCCs, inasmuch as vaccinal components and adjuvants can be easily obtained as clinical grade reagents.
Keywords: Head and neck squamous cell-carcinomas;; intra-cheek route; mucosal immunization; plasmo virus-like particles; pre-clinical orthotopic model; therapeutic vaccines; tumor microenvironment.
Figures
Similar articles
-
Intramuscular vaccination targeting mucosal tumor draining lymph node enhances integrins-mediated CD8+ T cell infiltration to control mucosal tumor growth.Oncoimmunology. 2018 May 24;7(8):e1463946. doi: 10.1080/2162402X.2018.1463946. eCollection 2018. Oncoimmunology. 2018. PMID: 30221059 Free PMC article.
-
Efficacy of DNA vaccines forming e7 recombinant retroviral virus-like particles for the treatment of human papillomavirus-induced cancers.Hum Gene Ther. 2013 May;24(5):533-44. doi: 10.1089/hum.2012.037. Epub 2013 May 6. Hum Gene Ther. 2013. PMID: 23521528
-
Natural killer T cell and TLR9 agonists as mucosal adjuvants for sublingual vaccination with clade C HIV-1 envelope protein.Vaccine. 2014 Dec 5;32(51):6934-6940. doi: 10.1016/j.vaccine.2014.10.051. Epub 2014 Nov 2. Vaccine. 2014. PMID: 25444819 Free PMC article.
-
Heterogeneity of the Head and Neck Squamous Cell Carcinoma Immune Landscape and Its Impact on Immunotherapy.Front Cell Dev Biol. 2019 Apr 9;7:52. doi: 10.3389/fcell.2019.00052. eCollection 2019. Front Cell Dev Biol. 2019. PMID: 31024913 Free PMC article. Review.
-
Human papillomavirus vaccines.Semin Cancer Biol. 1999 Dec;9(6):431-44. doi: 10.1006/scbi.1999.0147. Semin Cancer Biol. 1999. PMID: 10712890 Review.
Cited by
-
Toll-like receptor-targeted anti-tumor therapies: Advances and challenges.Front Immunol. 2022 Nov 21;13:1049340. doi: 10.3389/fimmu.2022.1049340. eCollection 2022. Front Immunol. 2022. PMID: 36479129 Free PMC article. Review.
-
Trial Watch: Toll-like receptor agonists in cancer immunotherapy.Oncoimmunology. 2018 Oct 11;7(12):e1526250. doi: 10.1080/2162402X.2018.1526250. eCollection 2018. Oncoimmunology. 2018. PMID: 30524908 Free PMC article. Review.
-
Naringenin potentiates anti-tumor immunity against oral cancer by inducing lymph node CD169-positive macrophage activation and cytotoxic T cell infiltration.Cancer Immunol Immunother. 2022 Sep;71(9):2127-2139. doi: 10.1007/s00262-022-03149-w. Epub 2022 Jan 19. Cancer Immunol Immunother. 2022. PMID: 35044489 Free PMC article.
-
Intramuscular vaccination targeting mucosal tumor draining lymph node enhances integrins-mediated CD8+ T cell infiltration to control mucosal tumor growth.Oncoimmunology. 2018 May 24;7(8):e1463946. doi: 10.1080/2162402X.2018.1463946. eCollection 2018. Oncoimmunology. 2018. PMID: 30221059 Free PMC article.
-
An Albumin-Binding Domain Peptide Confers Enhanced Immunoprotection Against Viral Myocarditis by CVB3 VP1 Vaccine.Front Immunol. 2021 Sep 22;12:666594. doi: 10.3389/fimmu.2021.666594. eCollection 2021. Front Immunol. 2021. PMID: 34630378 Free PMC article.
References
-
- Islami F, Fedirko V, Tramacere I, Bagnardi V, Jenab M, Scotti L, Rota M, Corrao G, Garavello W, Schuz J et al.. Alcohol drinking and esophageal squamous cell carcinoma with focus on light-drinkers and never-smokers: a systematic review and meta-analysis. Int J Cancer J Int Du Cancer 2011; 129:2473-84; PMID:21190191; http://dx.doi.org/2044464110.1002/ijc.25885 - DOI - PubMed
-
- Tramacere I, Negri E, Bagnardi V, Garavello W, Rota M, Scotti L, Islami F, Corrao G, Boffetta P, La Vecchia C. A meta-analysis of alcohol drinking and oral and pharyngeal cancers. Part 1: overall results and dose-risk relation. Oral Oncol 2010; 46:497-503; PMID:20444641; http://dx.doi.org/10.1016/j.oraloncology.2010.03.024 - DOI - PubMed
-
- Majchrzak E, Szybiak B, Wegner A, Pienkowski P, Pazdrowski J, Luczewski L, Sowka M, Golusinski P, Malicki J, Golusinski W. Oral cavity and oropharyngeal squamous cell carcinoma in young adults: a review of the literature. Radiol Oncol 2014; 48:1-10; PMID:24587773; http://dx.doi.org/10.2478/raon-2013-0057 - DOI - PMC - PubMed
-
- Fakhry C, Psyrri A, Chaturvedhi A. HPV and head and neck cancers: state-of-the-science. Oral Oncol 2014; 50:353-5; PMID:24726207; http://dx.doi.org/10.1016/j.oraloncology.2014.03.010 - DOI - PubMed
-
- Ho AS, Kraus DH, Ganly I, Lee NY, Shah JP, Morris LG. Decision making in the management of recurrent head and neck cancer. Head Neck 2014; 36:144-51; PMID:23471843; http://dx.doi.org/10.1002/hed.23227 - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials