

Plasma Chromogranin A as a marker of cardiovascular involvement in Erdheim-Chester disease
- PMID: 27622037
- PMCID: PMC5006912
- DOI: 10.1080/2162402X.2016.1181244
Plasma Chromogranin A as a marker of cardiovascular involvement in Erdheim-Chester disease
Abstract
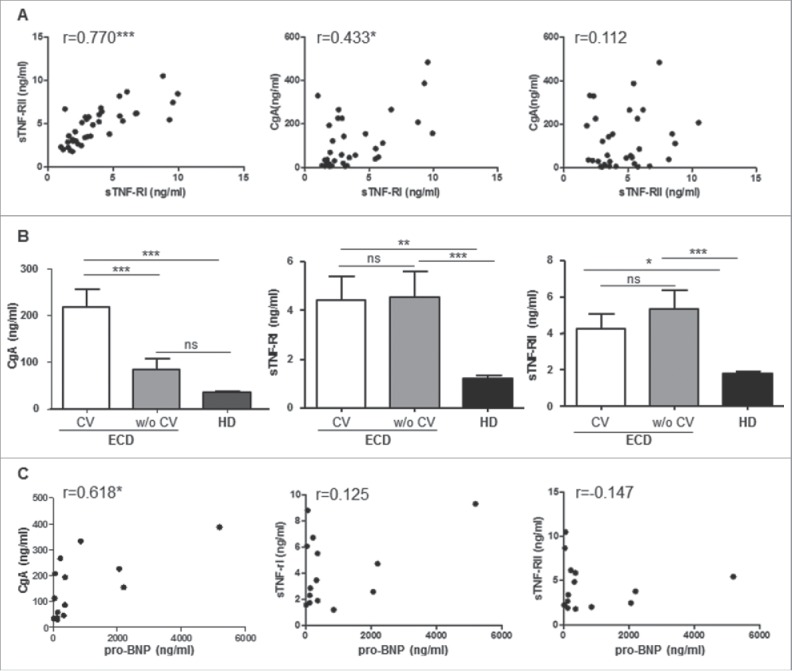
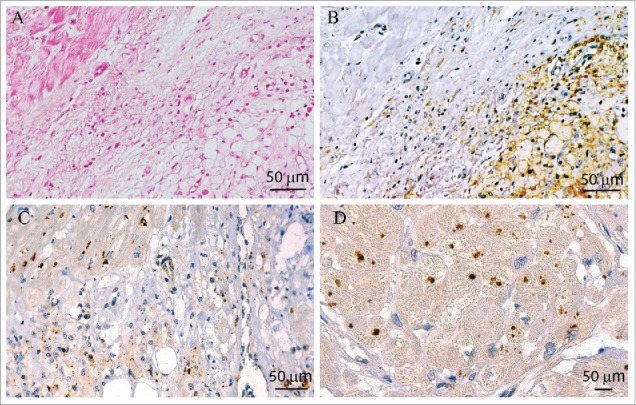
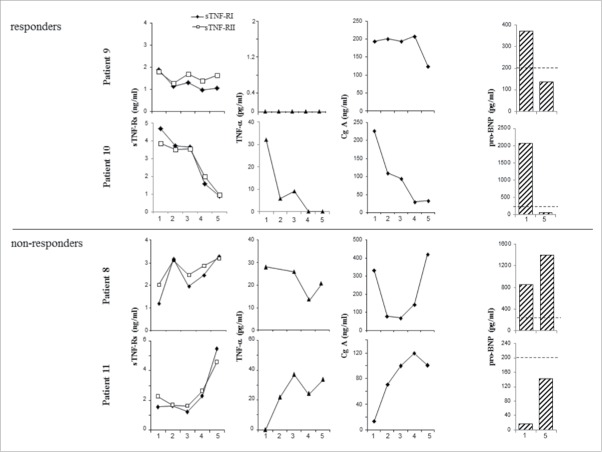
Erdheim-Chester disease (ECD) is a rare non-Langerhans cell histiocytosis (LCH) characterized by tissue infiltration with CD68(+) foamy histiocytes. TNF-related chronic inflammation and mutations in the MAP kinase signaling pathway in histiocytes are recognized as the two major pathogenic events. Among pleomorphic clinical manifestations, cardiovascular involvement is frequent and prognostically relevant. Evaluation of ECD clinical course and response to treatment is, however, still challenging. Taking advantage of the two largest cohorts of ECD patients worldwide, we investigated the relevance and the potential of circulating Chromogranin A (CgA), a pro-hormone involved in cardiovascular homeostasis and inflammation, as a biomarker of response to therapy in ECD. Consistent with other TNF-related inflammatory diseases, we found that not only TNF-α and soluble TNF-Receptors (sTNF-Rs), but also CgA plasma levels were significantly increased in ECD patients compared to controls. CgA, but not sTNF-Rs, discriminated cardiovascular involvement in ECD patients and correlated with pro-Brain Natriuretic Peptide (pro-BNP). In a single case, where a cardiac biopsy was available, CgA was found expressed by cardiomyocytes but not by infiltrating histiocytes. In four ECD patients, where serial determination of these parameters was obtained, the kinetics of sTNF-Rs and CgA paralleled response to therapy with anti-cytokine inhibitors; specifically, sTNF-Rs overlapped TNF-associated inflammation, while CgA, together with pro-BNP, closely mirrored response of cardiac disease. Our data indicate that both sTNF-Rs and CgA are linked to ECD pathophysiology. Moreover, CgA, in concert with pro-BNP, can be further exploited to fulfill the unmet clinical need of non-invasive reliable biomarkers of cardiac disease in these patients.
Keywords: Chromogranin A; Erdheim–Chester disease; TNF-α; chronic inflammation; histiocytes; soluble TNF-Receptors.
Figures
References
-
- Chester W. Über lipoidgranulomatose. Virchows Arch Pathol Anat Physiol Klin Med 1930; 279:561-602; http://dx.doi.org/10.1007/BF01942684 - DOI
-
- Veyssier-Belot C, Cacoub P, Caparros-Lefebvre D, Wechsler J, Brun B, Remy M, Wallaert B, Petit H, Grimaldi A, Wechsler B et al.. Erdheim-Chester disease. Clinical and radiologic characteristics of 59 cases. Medicine (Baltimore) 1996; 75:157-69; PMID:8965684; http://dx.doi.org/10.1097/00005792-199605000-00005 - DOI - PubMed
-
- Haroche J, Arnaud L, Amoura Z. Erdheim-Chester disease. Curr Opin Rheumatol 2012; 24:53-9; PMID:22089098; http://dx.doi.org/10.1097/BOR.0b013e32834d861d - DOI - PubMed
-
- Cavalli G, Guglielmi B, Berti A, Campochiaro C, Sabbadini MG, Dagna L. The multifaceted clinical presentations and manifestations of Erdheim-Chester disease: comprehensive review of the literature and of 10 new cases. Ann Rheum Dis 2013; 72:1691-5; PMID:23396641; http://dx.doi.org/10.1136/annrheumdis-2012-202542 - DOI - PubMed
-
- Diamond EL, Dagna L, Hyman DM, Cavalli G, Janku F, Estrada-Veras J, Ferrarini M, Abdel-Wahab O, Heaney ML, Scheel PJ et al.. Consensus guidelines for the diagnosis and clinical management of Erdheim-Chester disease. Blood 2014; 124:483-926; PMID:24850756; http://dx.doi.org/10.1182/blood-2014-03-561381 - DOI - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials