

The Effects of Pre-Existing Hyponatremia and Subsequent-Developing Acute Kidney Injury on In-Hospital Mortality: A Retrospective Cohort Study
- PMID: 27622451
- PMCID: PMC5021268
- DOI: 10.1371/journal.pone.0162990
The Effects of Pre-Existing Hyponatremia and Subsequent-Developing Acute Kidney Injury on In-Hospital Mortality: A Retrospective Cohort Study
Abstract
Background and objectives: Both hyponatremia and acute kidney injury (AKI) are common and harmful in hospitalized patients. However, their combined effects on patient mortality have been little studied.
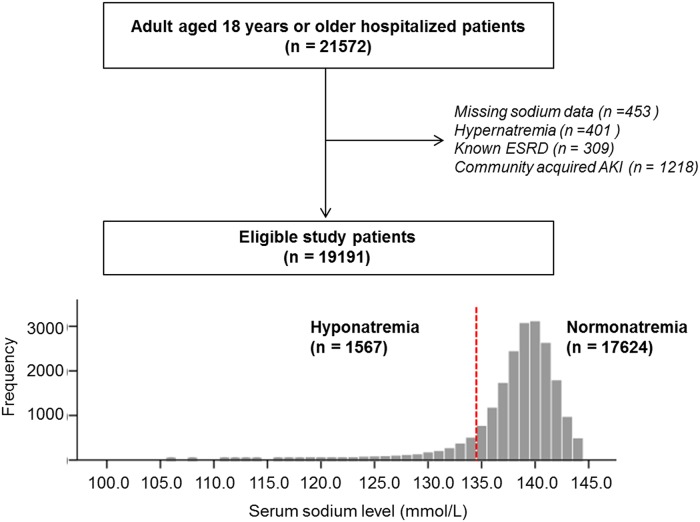
Methods: We retrospectively enrolled 19191 adult patients who were admitted for 1 year. Pre-existing hyponatremia was defined as a serum sodium level < 135 mmol/L on the first measurement of their admission. AKI was defined as a rise in serum creatinine by ≥ 26.5 μmol/L or ≥ 1.5 times of the baseline value of creatinine during the hospital stay.
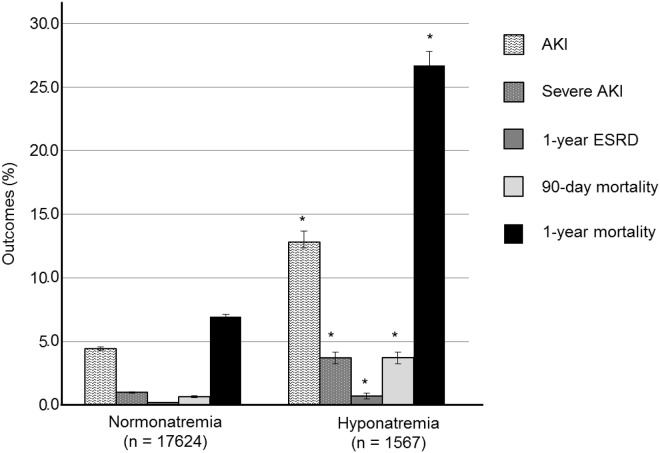
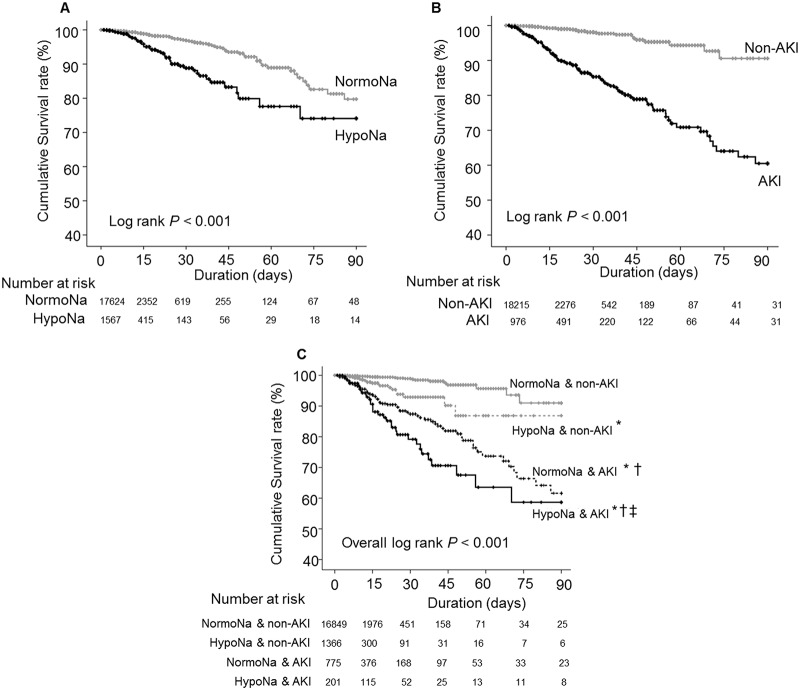
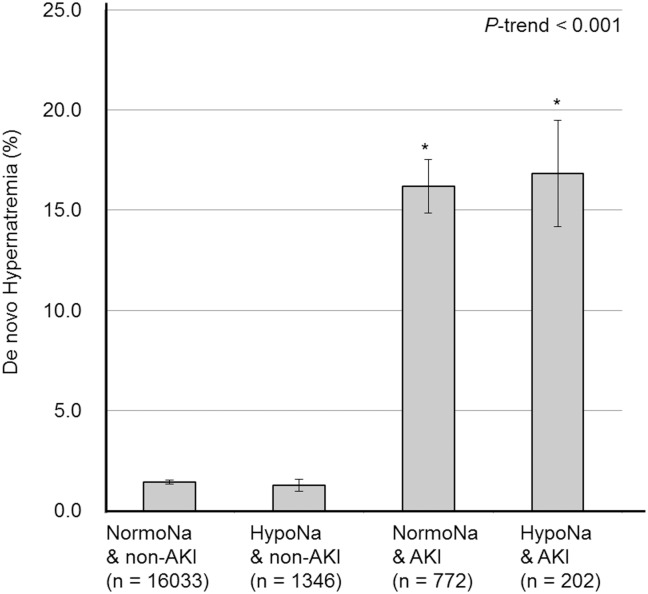
Results: The prevalence of pre-existing hyponatremia was 8.2%. During a median 6.0 days of hospital stay, the incidence rates of AKI and in-hospital patient mortality were 5.1% and 0.9%, respectively. Pre-existing hyponatremia independently predicted AKI development and in-hospital mortality (adjusted hazard ratio [HR] 1.300, P = 0.004; HR 2.481, P = 0.002, respectively). Pre-existing hyponatremia and subsequent development of AKI increased in-hospital mortality by 85 times, compared to the patients with normonatremia and no AKI. In subgroup analysis, the AKI group showed higher rates of de novo hypernatremia than the non-AKI group during the admission. De novo hypernatremia, which might be associated with over-correction of hyponatremia, increased in-hospital mortality (HR 3.297, P <0.001), and patients with AKI showed significantly higher rates of de novo hypernatremia than patients without AKI (16.2% vs. 1.4%, P < 0.001, respectively).
Conclusion: Pre-existing hyponatremia may be associated with the development of AKI in hospitalized patients, and both hyponatremia and hospital-acquired AKI could have a detrimental effect on short term patient mortality, which might be related to the inappropriate correction of hyponatremia in AKI patients.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
