

Scheduled Intermittent Screening with Rapid Diagnostic Tests and Treatment with Dihydroartemisinin-Piperaquine versus Intermittent Preventive Therapy with Sulfadoxine-Pyrimethamine for Malaria in Pregnancy in Malawi: An Open-Label Randomized Controlled Trial
- PMID: 27622558
- PMCID: PMC5021271
- DOI: 10.1371/journal.pmed.1002124
Scheduled Intermittent Screening with Rapid Diagnostic Tests and Treatment with Dihydroartemisinin-Piperaquine versus Intermittent Preventive Therapy with Sulfadoxine-Pyrimethamine for Malaria in Pregnancy in Malawi: An Open-Label Randomized Controlled Trial
Abstract
Background: In Africa, most plasmodium infections during pregnancy remain asymptomatic, yet are associated with maternal anemia and low birthweight. WHO recommends intermittent preventive therapy in pregnancy with sulfadoxine-pyrimethamine (IPTp-SP). However, sulfadoxine-pyrimethamine (SP) efficacy is threatened by high-level parasite resistance. We conducted a trial to evaluate the efficacy and safety of scheduled intermittent screening with malaria rapid diagnostic tests (RDTs) and treatment of RDT-positive women with dihydroartemisinin-piperaquine (DP) as an alternative strategy to IPTp-SP.
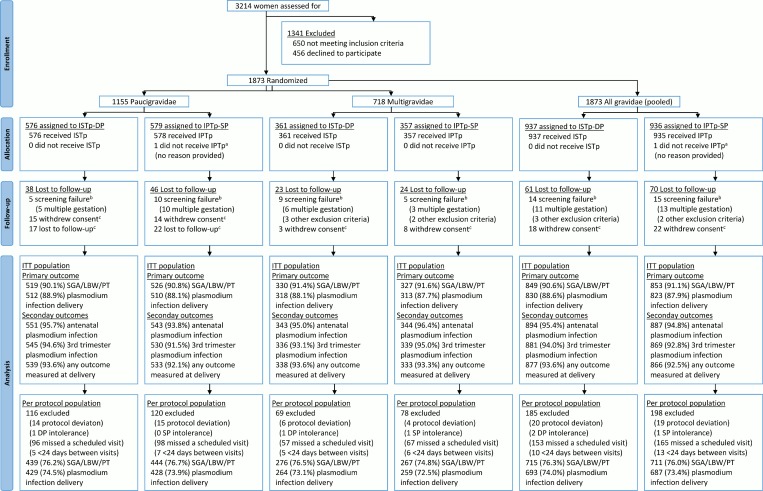
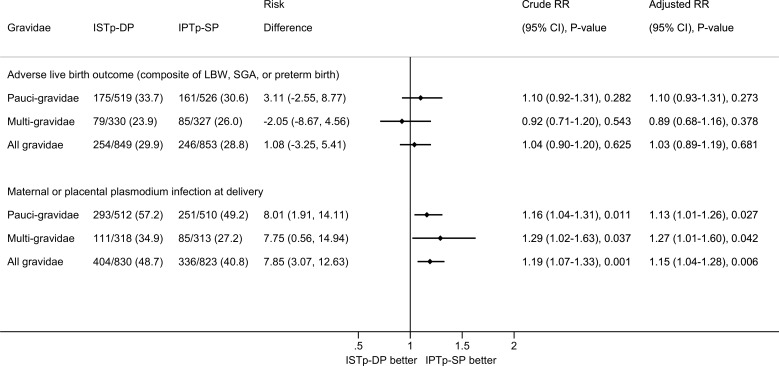
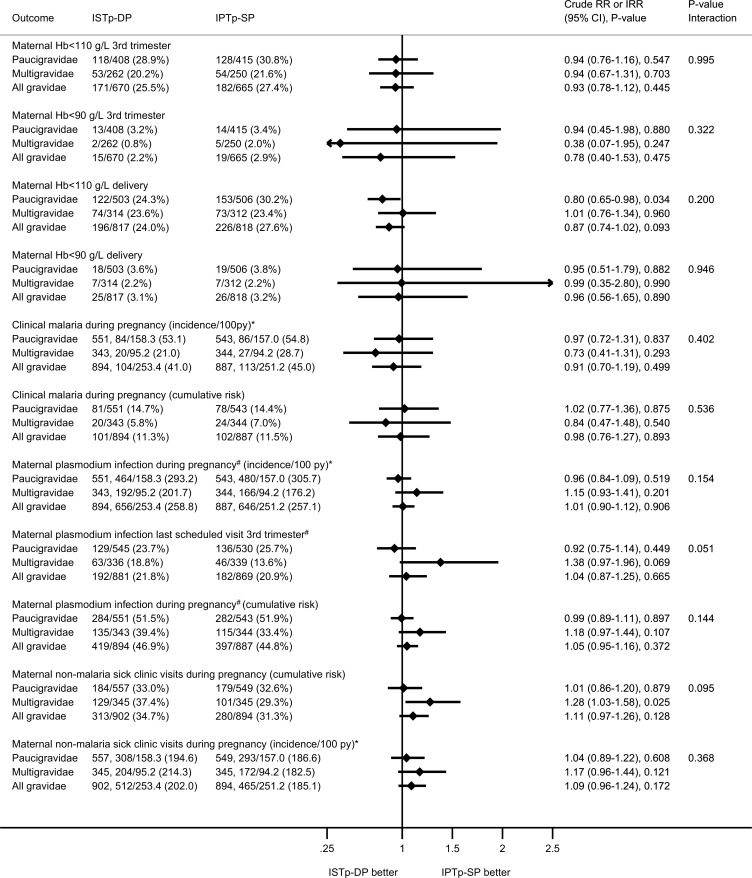
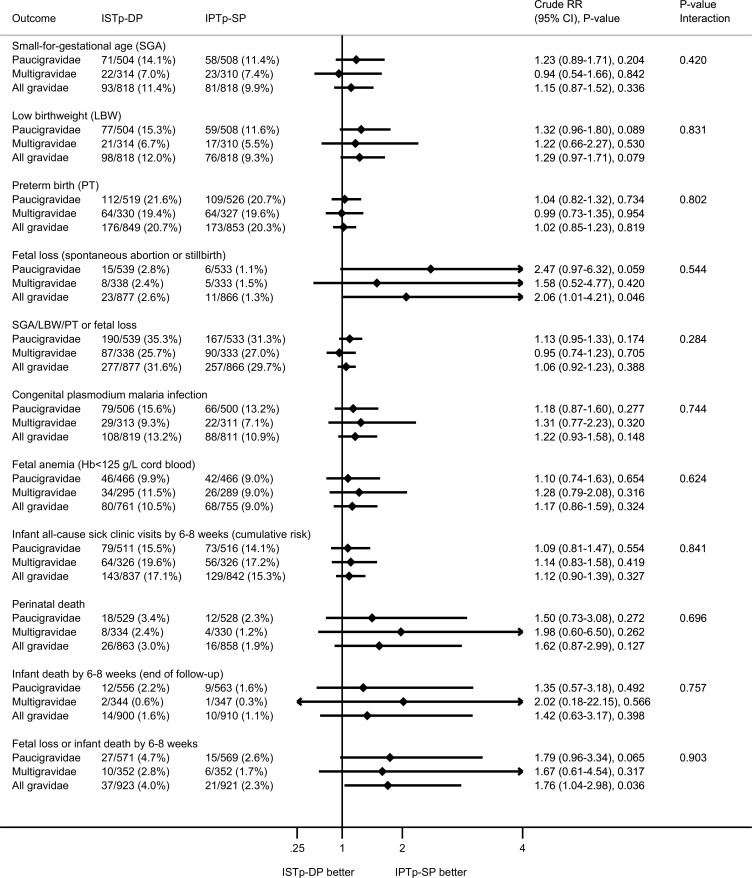
Methods and findings: This was an open-label, two-arm individually randomized superiority trial among HIV-seronegative women at three sites in Malawi with high SP resistance. The intervention consisted of three or four scheduled visits in the second and third trimester, 4 to 6 wk apart. Women in the IPTp-SP arm received SP at each visit. Women in the intermittent screening and treatment in pregnancy with DP (ISTp-DP) arm were screened for malaria at every visit and treated with DP if RDT-positive. The primary outcomes were adverse live birth outcome (composite of small for gestational age, low birthweight [<2,500 g], or preterm birth [<37 wk]) in paucigravidae (first or second pregnancy) and maternal or placental plasmodium infection at delivery in multigravidae (third pregnancy or higher). Analysis was by intention to treat. Between 21 July 2011 and 18 March 2013, 1,873 women were recruited (1,155 paucigravidae and 718 multigravidae). The prevalence of adverse live birth outcome was similar in the ISTp-DP (29.9%) and IPTp-SP (28.8%) arms (risk difference = 1.08% [95% CI -3.25% to 5.41%]; all women: relative risk [RR] = 1.04 [95% CI 0.90-1.20], p = 0.625; paucigravidae: RR = 1.10 [95% CI 0.92-1.31], p = 0.282; multigravidae: RR = 0.92 [95% CI 0.71-1.20], p = 0.543). The prevalence of malaria at delivery was higher in the ISTp-DP arm (48.7% versus 40.8%; risk difference = 7.85%, [95% CI 3.07%-12.63%]; all women: RR = 1.19 [95% CI 1.07-1.33], p = 0.007; paucigravidae: RR = 1.16 [95% CI 1.04-1.31], p = 0.011; multigravidae: RR = 1.29 [95% CI 1.02-1.63], p = 0.037). Fetal loss was more common with ISTp-DP (2.6% versus 1.3%; RR = 2.06 [95% CI 1.01-4.21], p = 0.046) and highest among non-DP-recipients (3.1%) in the ISTp-DP arm. Limitations included the open-label design.
Conclusions: Scheduled screening for malaria parasites with the current generation of RDTs three to four times during pregnancy as part of focused antenatal care was not superior to IPTp-SP in this area with high malaria transmission and high SP resistance and was associated with higher fetal loss and more malaria at delivery.
Trial registration: Pan African Clinical Trials Registry PACTR201103000280319; ISRCTN Registry ISRCTN69800930.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Desai M, Gutman J, Taylor SM, Wiegand RE, Khairallah C, Kayentao K, et al. Impact of sulfadoxine-pyrimethamine resistance on effectiveness of intermittent preventive therapy for malaria in pregnancy at clearing infections and preventing low birth weight. Clin Infect Dis. 2016;62:323–333. 10.1093/cid/civ881 - DOI - PMC - PubMed
-
- Chico RM, Cano J, Ariti C, Collier TJ, Chandramohan D, Roper C, et al. Influence of malaria transmission intensity and the 581G mutation on the efficacy of intermittent preventive treatment in pregnancy: systematic review and meta-analysis. Trop Med Int Health. 2015;20:1621–1633. 10.1111/tmi.12595 - DOI - PubMed
-
- Harrington WE, Mutabingwa TK, Muehlenbachs A, Sorensen B, Bolla MC, Fried M, et al. Competitive facilitation of drug-resistant Plasmodium falciparum malaria parasites in pregnant women who receive preventive treatment. Proc Natl Acad Sci U S A. 2009;106:9027–9032. 10.1073/pnas.0901415106 - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
