

The extracellular matrix - the under-recognized element in lung disease?
- PMID: 27623753
- PMCID: PMC5129494
- DOI: 10.1002/path.4808
The extracellular matrix - the under-recognized element in lung disease?
Abstract
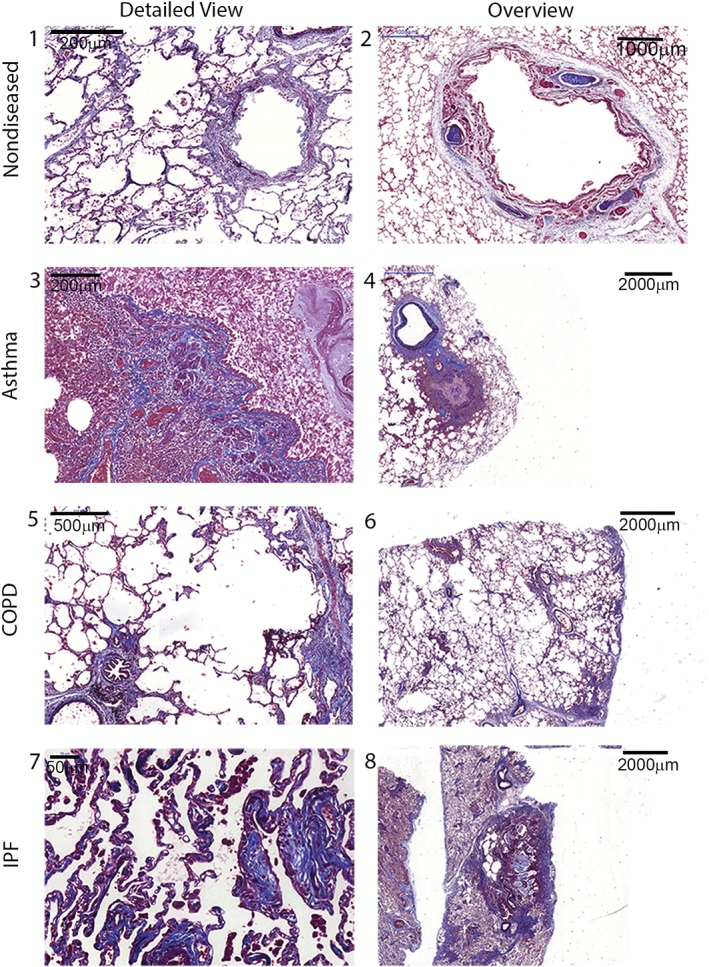
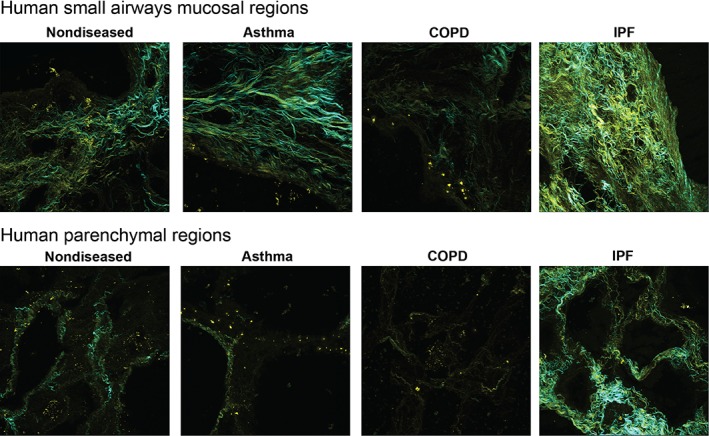
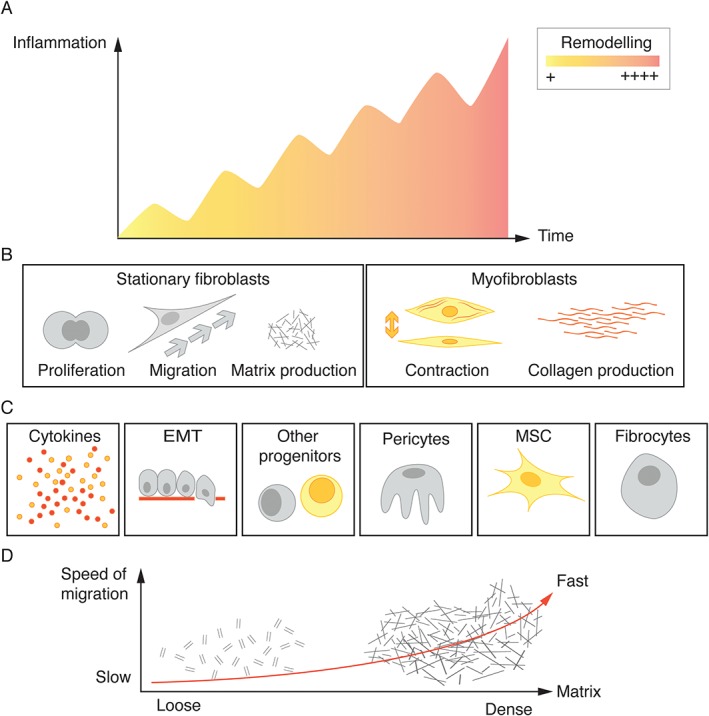
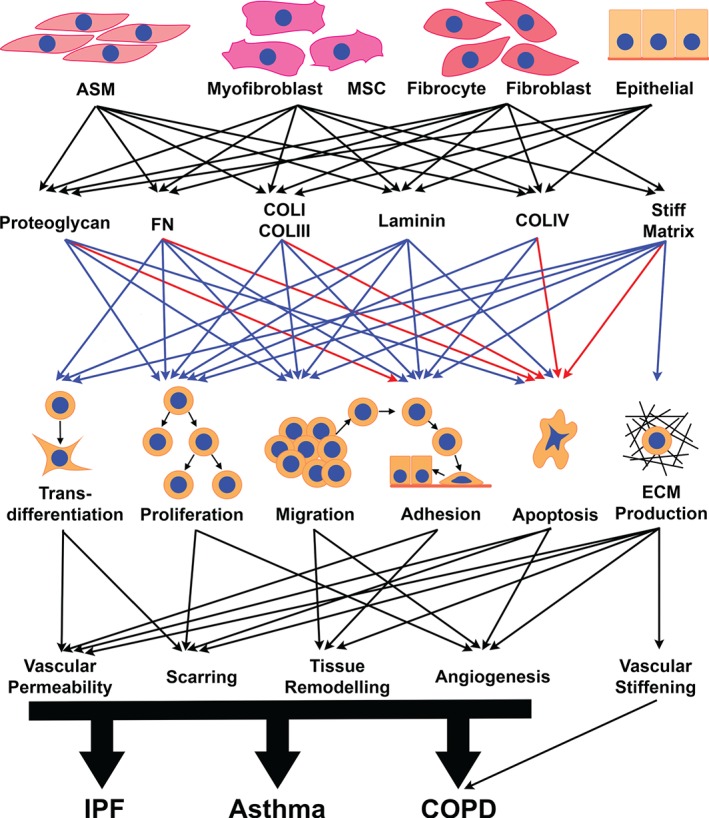
The lung is composed of airways and lung parenchyma, and the extracellular matrix (ECM) contains the main building blocks of both components. The ECM provides physical support and stability to the lung, and as such it has in the past been regarded as an inert structure. More recent research has provided novel insights revealing that the ECM is also a bioactive environment that orchestrates the cellular responses in its environs. Changes in the ECM in the airway or parenchymal tissues are now recognized in the pathological profiles of many respiratory diseases, including asthma, chronic obstructive pulmonary disease (COPD), and idiopathic pulmonary fibrosis (IPF). Only recently have we begun to investigate whether these ECM changes result from the disease process, or whether they constitute a driving factor that orchestrates the pathological outcomes. This review summarizes our current knowledge of the alterations in the ECM in asthma, COPD, and IPF, and the contributions of these alterations to the pathologies. Emerging data suggest that alterations in the composition, folding or rigidity of ECM proteins may alter the functional responses of cells within their environs, and in so doing change the pathological outcomes. These characteristics highlight potential avenues for targeting lung pathologies in the future. This may ultimately contribute to a better understanding of chronic lung diseases, and novel approaches for finding therapeutic solutions. © 2016 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Keywords: asthma; chronic obstructive pulmonary disease; collagen; extracellular matrix; fibrosis; lung; myofibroblast; niche.
© 2016 The Authors. The Journal of Pathology published by John Wiley & Sons Ltd on behalf of Pathological Society of Great Britain and Ireland.
Figures

References
-
- Huber HL, Koessler KK. The pathology of bronchial asthma. Arch Intern Med 1922; 30 : 689–760.
-
- Roche WR, Beasley R, Williams JH, et al. Subepithelial fibrosis in the bronchi of asthmatics. Lancet 1989; 1: 520–524. - PubMed
-
- Jeffery PK, Wardlaw AJ, Nelson FC, et al. Bronchial biopsies in asthma. An ultrastructural, quantitative study and correlation with hyperreactivity. Am Rev Respir Dis 1989; 140: 1745–1753. - PubMed
-
- Broekema M, Timens W, Vonk JM, et al. Persisting remodeling and less airway wall eosinophil activation in complete remission of asthma. Am J Respir Crit Care Med 2011; 183: 310–316. - PubMed
-
- Payne DN, Rogers AV, Adelroth E, et al. Early thickening of the reticular basement membrane in children with difficult asthma. Am J Respir Crit Care Med 2003; 167: 78–82. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
