

Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis
- PMID: 27624087
- PMCID: PMC5021824
- DOI: 10.1136/bmj.i4694
Hyperglycaemia and risk of adverse perinatal outcomes: systematic review and meta-analysis
Abstract
Objectives: To assess the association between maternal glucose concentrations and adverse perinatal outcomes in women without gestational or existing diabetes and to determine whether clear thresholds for identifying women at risk of perinatal outcomes can be identified.
Design: Systematic review and meta-analysis of prospective cohort studies and control arms of randomised trials.
Data sources: Databases including Medline and Embase were searched up to October 2014 and combined with individual participant data from two additional birth cohorts.
Eligibility criteria for selecting studies: Studies including pregnant women with oral glucose tolerance (OGTT) or challenge (OGCT) test results, with data on at least one adverse perinatal outcome.
Appraisal and data extraction: Glucose test results were extracted for OGCT (50 g) and OGTT (75 g and 100 g) at fasting and one and two hour post-load timings. Data were extracted on induction of labour; caesarean and instrumental delivery; pregnancy induced hypertension; pre-eclampsia; macrosomia; large for gestational age; preterm birth; birth injury; and neonatal hypoglycaemia. Risk of bias was assessed with a modified version of the critical appraisal skills programme and quality in prognostic studies tools.
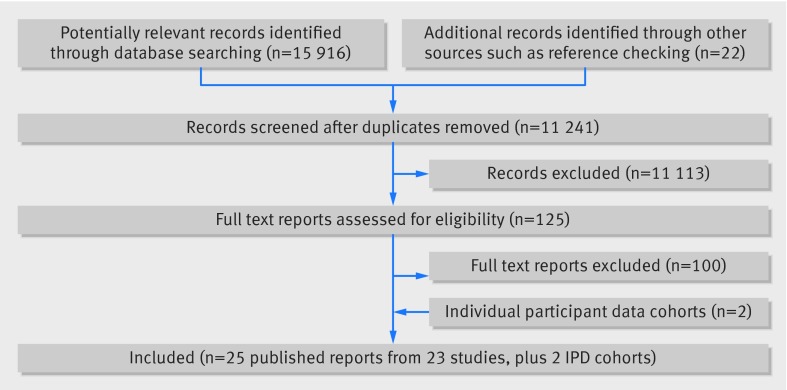
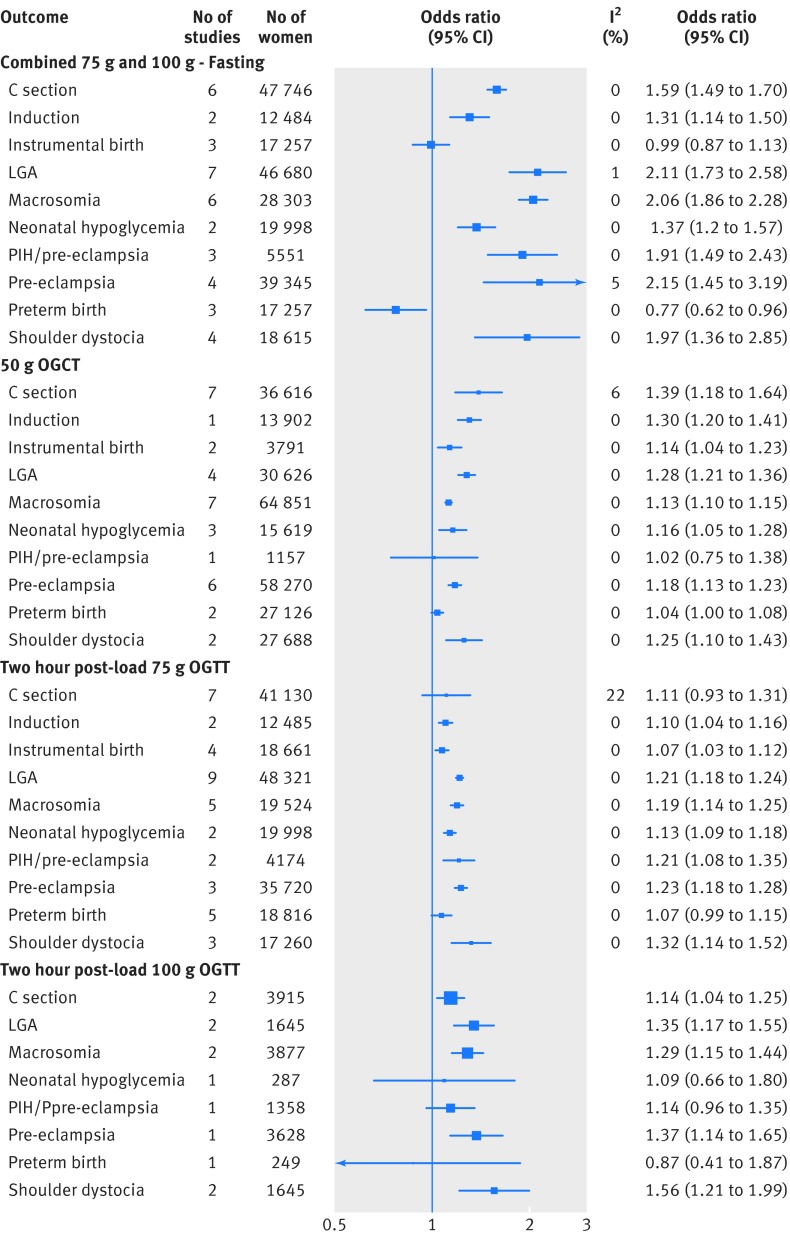
Results: 25 reports from 23 published studies and two individual participant data cohorts were included, with up to 207 172 women (numbers varied by the test and outcome analysed in the meta-analyses). Overall most studies were judged as having a low risk of bias. There were positive linear associations with caesarean section, induction of labour, large for gestational age, macrosomia, and shoulder dystocia for all glucose exposures across the distribution of glucose concentrations. There was no clear evidence of a threshold effect. In general, associations were stronger for fasting concentration than for post-load concentration. For example, the odds ratios for large for gestational age per 1 mmol/L increase of fasting and two hour post-load glucose concentrations (after a 75 g OGTT) were 2.15 (95% confidence interval 1.60 to 2.91) and 1.20 (1.13 to 1.28), respectively. Heterogeneity was low between studies in all analyses.
Conclusions: This review and meta-analysis identified a large number of studies in various countries. There was a graded linear association between fasting and post-load glucose concentration across the whole glucose distribution and most adverse perinatal outcomes in women without pre-existing or gestational diabetes. The lack of a clear threshold at which risk increases means that decisions regarding thresholds for diagnosing gestational diabetes are somewhat arbitrary. Research should now investigate the clinical and cost-effectiveness of applying different glucose thresholds for diagnosis of gestational diabetes on perinatal and longer term outcomes.
Systematic review registration: PROSPERO CRD42013004608.
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Conflict of interest statement
All authors have completed the ICMJE uniform disclosure form at www.icmje.org/coi_disclosure.pdf and declare: no support from any organisation for the submitted work; no financial relationships with any organisations that might have an interest in the submitted work in the previous three years; no other relationships or activities that could appear to have influenced the submitted work.
Figures
References
-
- Hartling L, Dryden DM, Guthrie A, Muise M, Vandermeer B, Donovan L. Benefits and harms of treating gestational diabetes mellitus: a systematic review and meta-analysis for the U.S. Preventive Services Task Force and the National Institutes of Health Office of Medical Applications of Research. Ann Intern Med 2013;159:123-9. 10.7326/0003-4819-159-2-201307160-00661 pmid:23712381. - DOI - PubMed
-
- Shah BR, Retnakaran R, Booth GL. Increased risk of cardiovascular disease in young women following gestational diabetes mellitus. Diabetes Care 2008;31:1668-9. 10.2337/dc08-0706 pmid:18487472. - DOI - PMC - PubMed
-
- Boney CM, Verma A, Tucker R, Vohr BR. Metabolic syndrome in childhood: association with birth weight, maternal obesity, and gestational diabetes mellitus. Pediatrics 2005;115:e290-6. 10.1542/peds.2004-1808 pmid:15741354. - DOI - PubMed
-
- Clausen TD, Mathiesen ER, Hansen T, et al. High prevalence of type 2 diabetes and pre-diabetes in adult offspring of women with gestational diabetes mellitus or type 1 diabetes: the role of intrauterine hyperglycemia. Diabetes Care 2008;31:340-6. 10.2337/dc07-1596 pmid:18000174. - DOI - PubMed
-
- Metzger BE, Gabbe SG, Persson B, et al. International Association of Diabetes and Pregnancy Study Groups Consensus Panel. International association of diabetes and pregnancy study groups recommendations on the diagnosis and classification of hyperglycemia in pregnancy. Diabetes Care 2010;33:676-82. 10.2337/dc10-0719 pmid:20190296. - DOI - PMC - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases