

Serum cystatin is a useful marker for the diagnosis of acute kidney injury in critically ill children: prospective cohort study
- PMID: 27624749
- PMCID: PMC5022154
- DOI: 10.1186/s12882-016-0346-z
Serum cystatin is a useful marker for the diagnosis of acute kidney injury in critically ill children: prospective cohort study
Abstract
Background: Acute kidney injury (AKI) has been associated with high morbidity and mortality rates among critically ill children. Cystatin C is a protease inhibitor, and studies have shown that it is a promising marker for the early diagnosis of AKI. Our goal in this study was to assess whether serum cystatin C could serve as an accurate marker for the diagnosis of AKI.
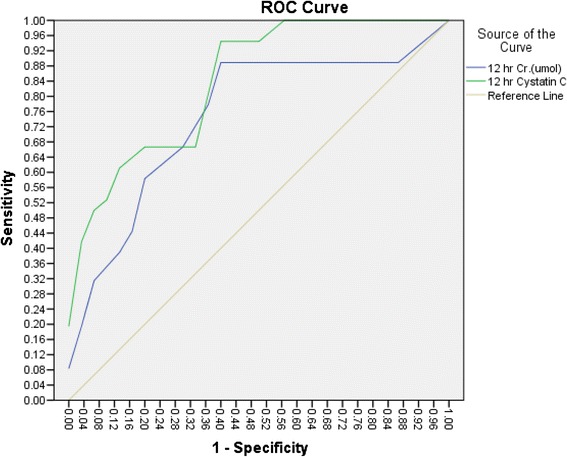
Methods: This prospective study was undertaken in the pediatric intensive care unit at King Abdulaziz University Hospital. Serum creatinine and serum cystatin C levels were both measured in patients on admission (0 h) and at 6, 12, and 24 h after admission. AKI was diagnosed according to the modified pRIFLE criteria. Receiver operating characteristic (ROC) curve analysis was performed to assess the utility of serum cystatin C for diagnosing AKI.
Results: A total of 62 patients were enrolled in this study, and 32 were diagnosed with AKI according to the modified pRIFLE criteria (51.4 %). The area under the ROC curve for serum cystatin indicated that it was a good marker for the diagnosis of AKI at 0, 6, 12 and 24 h, with sensitivities of 78, 94, 94 and 83 %, respectively. However, the specificities of serum cystatin C at 0, 6, 12, and 24 h were 57, 57, 60 and 50 %, respectively. The optimal cutoff value was 0.645 mg/L. The area under the ROC for serum creatinine showed sensitivities of 50, 65.4, 69.2 and 57.7 % and specificities of 67.7, 70, 60 and 70 % at 0, 6, 12 and 24 h, respectively. The optimal cutoff value for serum creatinine was 30 μmol/l. Comparisons of ROC curves revealed that serum cystatin C was superior to serum creatinine for the diagnosis of AKI at 12 h (p = 0.03), but no differences were detected at 0, 6 or 24 h.
Conclusion: Serum cystatin is a sensitive, but not a specific, marker for the diagnosis of AKI in critically ill children.
Keywords: Acute kidney injury; Creatinine; Cystatin C; Pediatric.
Figures



References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–12. doi: 10.1186/cc2872. - DOI - PMC - PubMed
-
- KDIGO Clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:8. doi: 10.1038/kisup.2012.7. - DOI
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
