

Review
doi: 10.1056/NEJMra1501993.
Biologic and Clinical Perspectives on Thyroid Cancer
Affiliations
- PMID: 27626519
- PMCID: PMC5512163
- DOI: 10.1056/NEJMra1501993
Item in Clipboard
Review
Biologic and Clinical Perspectives on Thyroid Cancer
N Engl J Med.
.
No abstract available
Figures
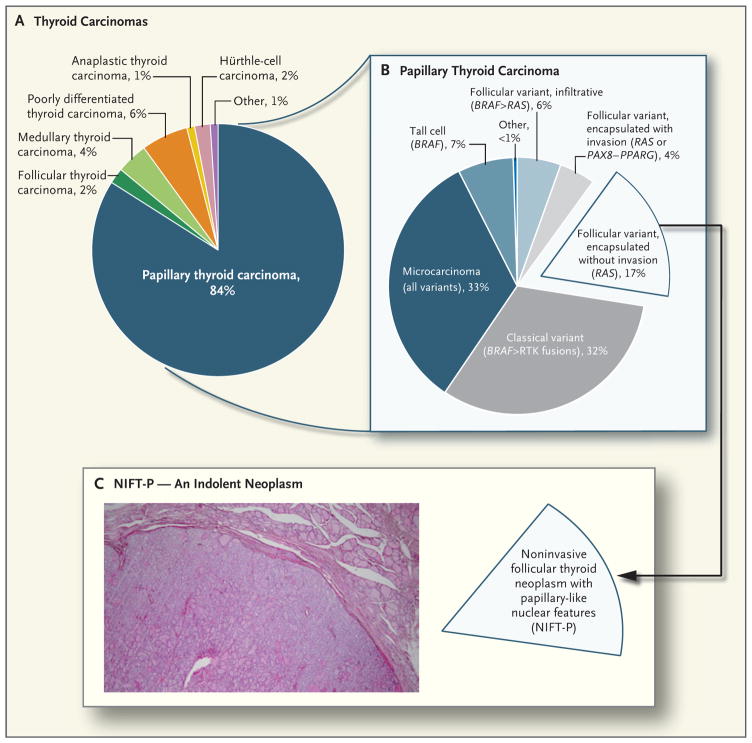
Panel A shows the relative incidence of the main types of thyroid cancer in the United States, and Panel B the relative frequency of pathologic variants of papillary thyroid carcinoma, with their corresponding main driver mutations shown in parentheses (the symbol > indicates more frequent than). RTK denotes receptor tyrosine kinase. Panel C shows the encapsulated follicular variant of papillary thyroid carcinoma without invasion, which until recently represented 17% of all papillary thyroid carcinomas. This cancer has recently been reclassified as a neoplasm of low malignant potential and is now termed “noninvasive follicular thyroid neoplasm with papillary−like nuclear features” (NIFT−P). This change will result in a corresponding reduction in the number of patients who are considered to have thyroid cancer. The hematoxylin and eosin–stained section in the inset shows the characteristic histologic appearance of an NIFT−P. The encapsulated tumor has a follicular growth pattern and papillary nuclear features, low mitotic rate, and absence of necrosis and capsular or vascular invasion.
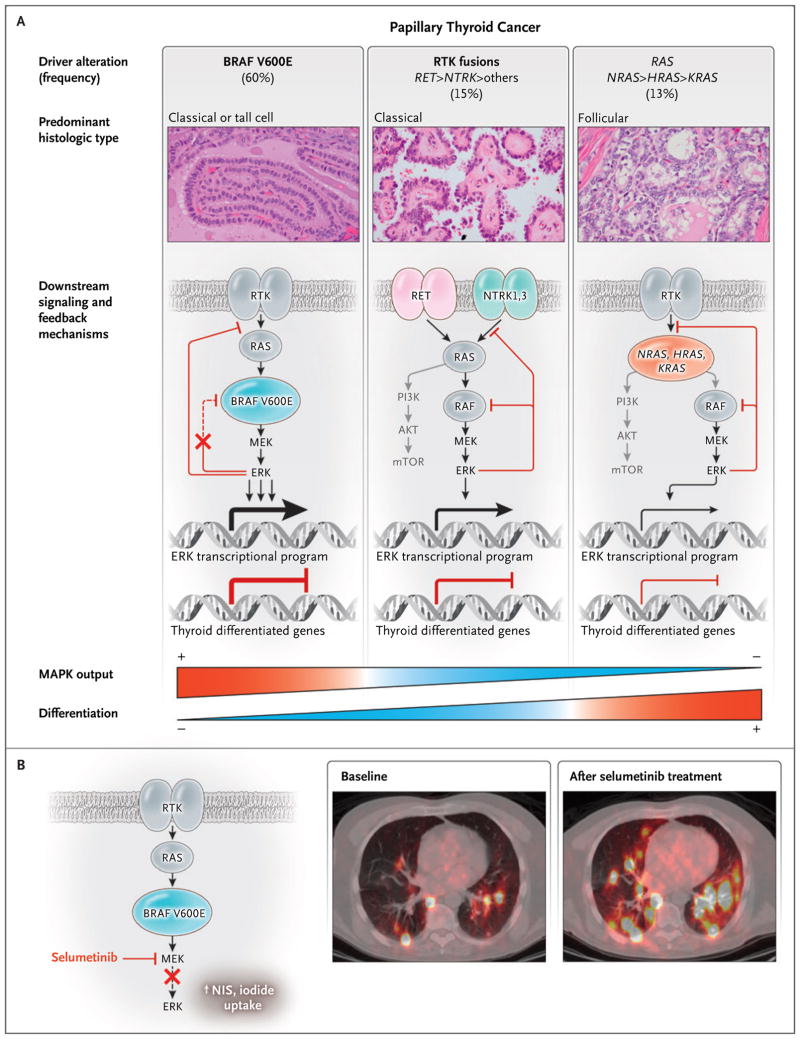
Panel A shows that papillary thyroid carcinomas have mutually exclusive activating mutations in BRAF, RAS, and RTK. The photomicrographs show hematoxylin and eosin–stained slides of the indicated variants of papillary thyroid carcinoma. Mutant RTKs, RAS, and BRAF activate mitogen−activated protein kinase (MAPK) signaling but do so to different degrees. The symbol > indicates more frequent than. The signaling output driven by BRAF V600E is highest, because this oncoprotein signals as a monomer and is unresponsive to the negative−feedback effects of activated ERK on upstream inputs into the pathway.– By contrast, the MAPK−signaling flux that is evoked by fusion RTK proteins or by mutated RAS is dampened by negative feedback. The expression of genes that is required for iodide uptake and metabolism, which are hallmarks of the differentiated state of thyroid follicular cells, is inhibited by MAPK signaling. This is consequential, because responsiveness to radioiodine therapy requires preservation of thyroid−differentiated function. The weight of the lines and arrows indicates the magnitude of the flux through the MAPK pathway and the transcriptional activities, respectively. The term mTOR denotes mammalian target of rapamycin, and PI3K phosphatidylinositol 3−kinase. Panel B (left side) shows that the MAPK kinase (MEK) inhibitor selumetinib decreases extracellular signal−regulated kinase (ERK) activation and restores expression of the sodium iodide transporter (NIS) and other thyroid differentiation genes in mice with Braf V600E–driven papillary thyroid carcinoma. The insets on the right side of Panel B are fused iodine−124 positron−emission tomographic–computed tomographic images showing the restoration of iodine−124 uptake with selumetinib treatment in a patient with radioiodine−refractory lung metastases of thyroid cancer. Adapted, with permission, from Ho et al.
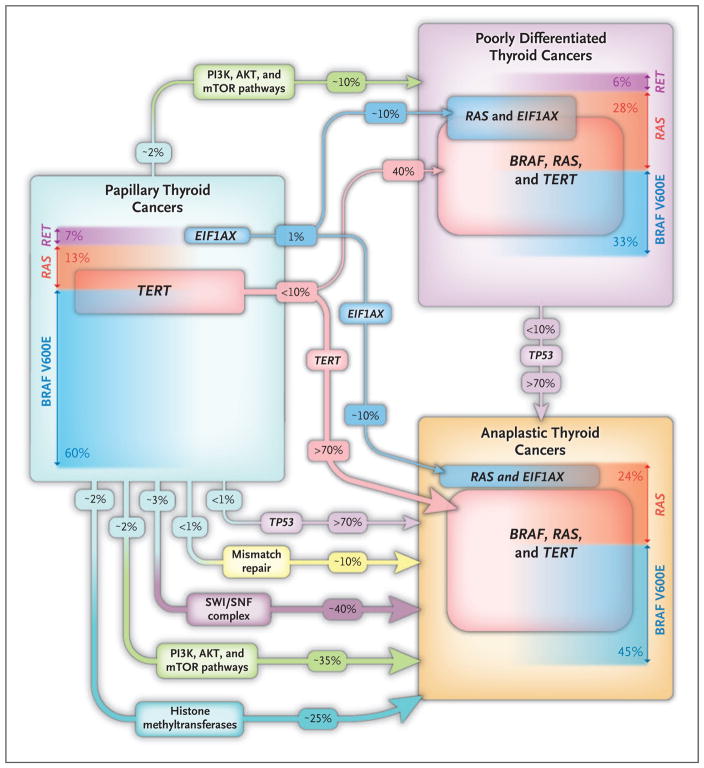
The frequency of the main somatic genetic defects in papillary, poorly differentiated, and anaplastic thyroid carcinoma is shown, based on the largest published series studied by next−generation sequencing., Because anaplastic thyroid carcinomas are extensively infiltrated by tumor−associated macrophages, deep sequencing is required to make reliable mutation calls. The prevalence of driver mutations (BRAF, RAS, and RET) in the histologic types of the three tumors is shown. In patients with advanced disease, tumors may have more than one mutation, so the overall mutation burden exceeds 100%. The frequency of the main drivers (BRAF, RAS, and RET) sums to less than 100% because in some cases the drivers are not known or they are lower−frequency events and are not listed here (e.g., NF1, PTEN). TERT promoter mutations appear to be key transitional steps in the microevolution of tumors. In papillary thyroid carcinoma, the TERT mutations are infrequent (in 10% of tumors) and usually subclonal. By contrast, their prevalence is substantially higher in poorly differentiated and anaplastic thyroid carcinomas, in which they are uniformly clonal. Mutations in TP53 are infrequent in all histologic types of thyroid cancer with the exception of anaplastic thyroid carcinomas, in which they occur in more than 70% of patients. Anaplastic thyroid carcinomas have mutations in genes encoding components of the PI3K–AKT–mTOR pathway and of proteins involved in epigenetic regulation, whereas poorly differentiated thyroid carcinomas have an intermediate frequency of these events (data not shown). Mutations of EIF1AX, a component of the translation preinitiation complex, are infrequent and are mutually exclusive with other driver mutations in papillary thyroid cancer. In poorly differentiated and anaplastic thyroid cancers, they are markedly enriched and are strongly associated with RAS−mutated tumors.
Comment in
-
Biologic and Clinical Perspectives on Thyroid Cancer.N Engl J Med. 2016 Dec 8;375(23):2307. doi: 10.1056/NEJMc1613118. N Engl J Med. 2016. PMID: 27959677 No abstract available.
-
Biologic and Clinical Perspectives on Thyroid Cancer.N Engl J Med. 2016 Dec 8;375(23):2306-2307. doi: 10.1056/NEJMc1613118. N Engl J Med. 2016. PMID: 27959678 No abstract available.
References
-
- Davies L, Welch HG. Current thyroid cancer trends in the United States. JAMA Otolaryngol Head Neck Surg. 2014;140:317–22. - PubMed
-
- Kimura ET, Nikiforova MN, Zhu Z, Knauf JA, Nikiforov YE, Fagin JA. High prevalence of BRAF mutations in thyroid cancer: genetic evidence for constitutive activation of the RET/PTC-RAS-BRAF signaling pathway in papillary thyroid carcinoma. Cancer Res. 2003;63:1454–7. - PubMed
-
- Xing M, Westra WH, Tufano RP, et al. BRAF mutation predicts a poorer clinical prognosis for papillary thyroid cancer. J Clin Endocrinol Metab. 2005;90:6373–9. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical