

HIV and cancer registry linkage identifies a substantial burden of cancers in persons with HIV in India
- PMID: 27631245
- PMCID: PMC5402588
- DOI: 10.1097/MD.0000000000004850
HIV and cancer registry linkage identifies a substantial burden of cancers in persons with HIV in India
Abstract
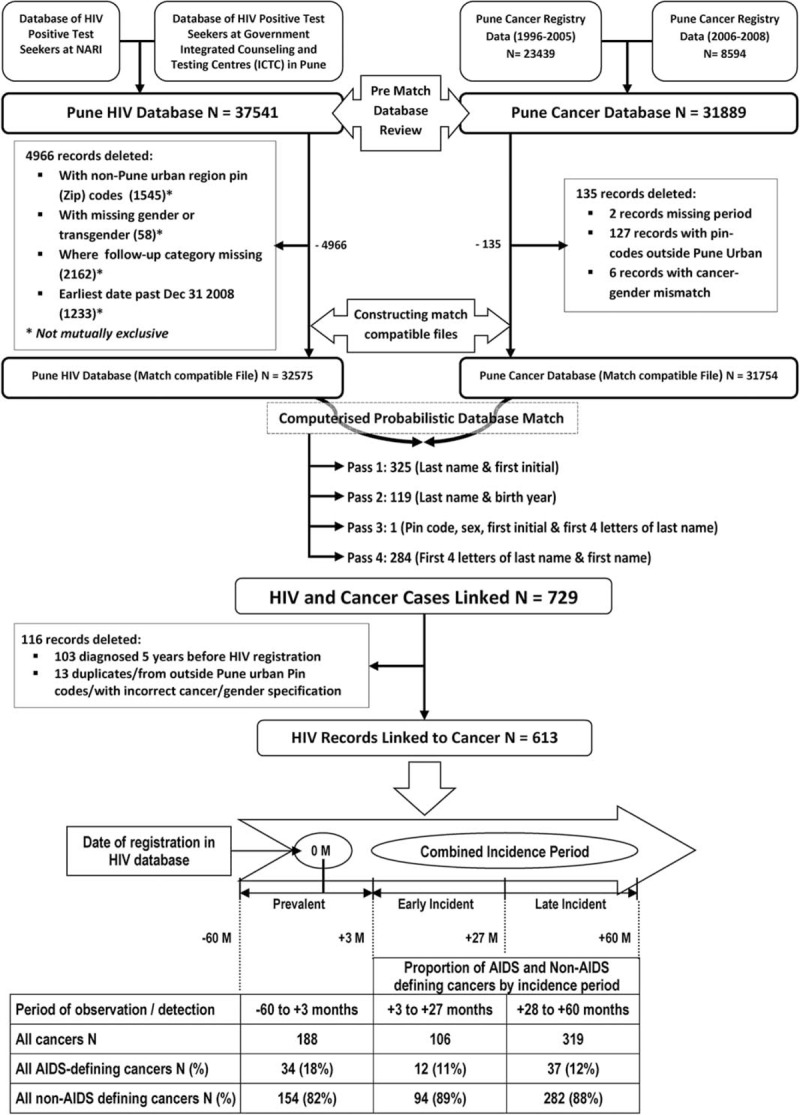
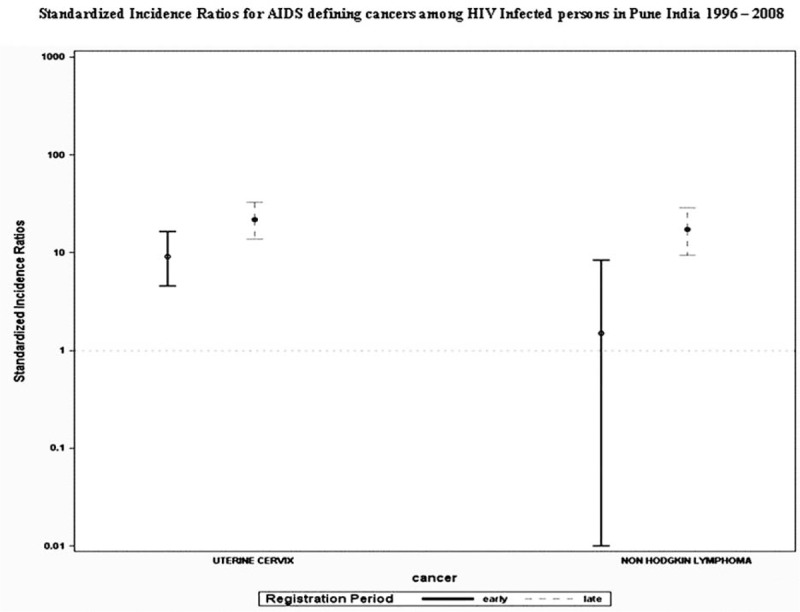
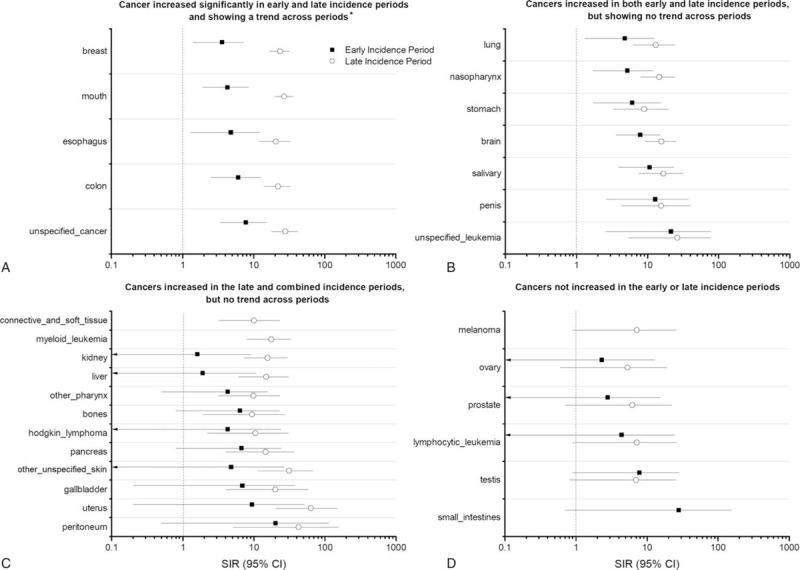
We utilized computerized record-linkage methods to link HIV and cancer databases with limited unique identifiers in Pune, India, to determine feasibility of linkage and obtain preliminary estimates of cancer risk in persons living with HIV (PLHIV) as compared with the general population.Records of 32,575 PLHIV were linked to 31,754 Pune Cancer Registry records (1996-2008) using a probabilistic-matching algorithm. Cancer risk was estimated by calculating standardized incidence ratios (SIRs) in the early (4-27 months after HIV registration), late (28-60 months), and overall (4-60 months) incidence periods. Cancers diagnosed prior to or within 3 months of HIV registration were considered prevalent.Of 613 linked cancers to PLHIV, 188 were prevalent, 106 early incident, and 319 late incident. Incident cancers comprised 11.5% AIDS-defining cancers (ADCs), including cervical cancer and non-Hodgkin lymphoma (NHL), but not Kaposi sarcoma (KS), and 88.5% non-AIDS-defining cancers (NADCs). Risk for any incident cancer diagnosis in early, late, and combined periods was significantly elevated among PLHIV (SIRs: 5.6 [95% CI 4.6-6.8], 17.7 [95% CI 15.8-19.8], and 11.5 [95% CI 10-12.6], respectively). Cervical cancer risk was elevated in both incidence periods (SIRs: 9.6 [95% CI 4.8-17.2] and 22.6 [95% CI 14.3-33.9], respectively), while NHL risk was elevated only in the late incidence period (SIR: 18.0 [95% CI 9.8-30.20]). Risks for NADCs were dramatically elevated (SIR > 100) for eye-orbit, substantially (SIR > 20) for all-mouth, esophagus, breast, unspecified-leukemia, colon-rectum-anus, and other/unspecified cancers; moderately elevated (SIR > 10) for salivary gland, penis, nasopharynx, and brain-nervous system, and mildly elevated (SIR > 5) for stomach. Risks for 6 NADCs (small intestine, testis, lymphocytic leukemia, prostate, ovary, and melanoma) were not elevated and 5 cancers, including multiple myeloma not seen.Our study demonstrates the feasibility of using probabilistic record-linkage to study cancer/other comorbidities among PLHIV in India and provides preliminary population-based estimates of cancer risks in PLHIV in India. Our results, suggesting a potentially substantial burden and slightly different spectrum of cancers among PLHIV in India, support efforts to conduct multicenter linkage studies to obtain precise estimates and to monitor cancer risk in PLHIV in India.
Conflict of interest statement
None of the authors has any conflicts of interest to declare for this manuscript.
Figures
References
-
- NACO. Technical Report on HIV Estimation. 2006
-
- NACO. India HIV Estimations 2015. 2015
-
- NACO. Annual Report 2014-15. 2015
-
- Engels EA, Pfeiffer RM, Goedert JJ, et al. Trends in cancer risk among people with AIDS in the United States 1980-2002. AIDS 2006; 20:1645–1654. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
