

Different surgical strategies of patients with intravenous leiomyomatosis
- PMID: 27631266
- PMCID: PMC5402609
- DOI: 10.1097/MD.0000000000004902
Different surgical strategies of patients with intravenous leiomyomatosis
Abstract
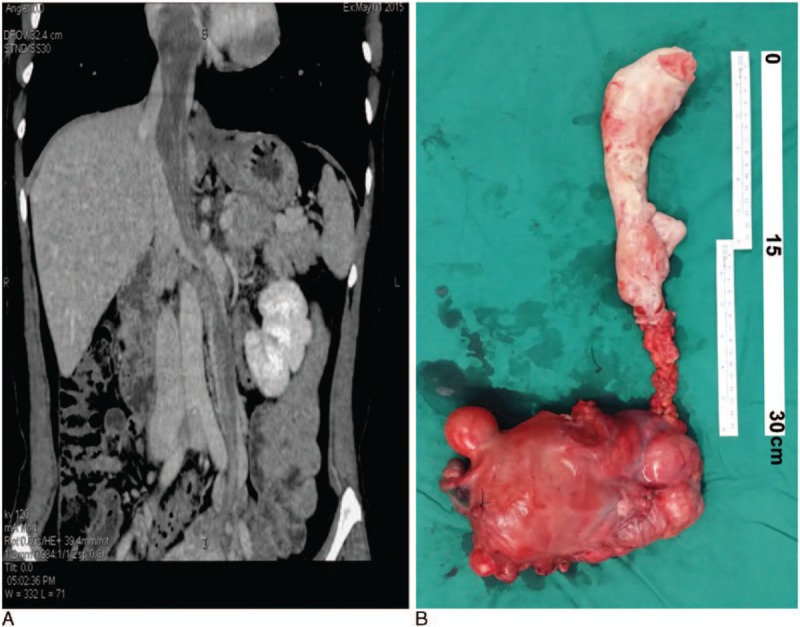
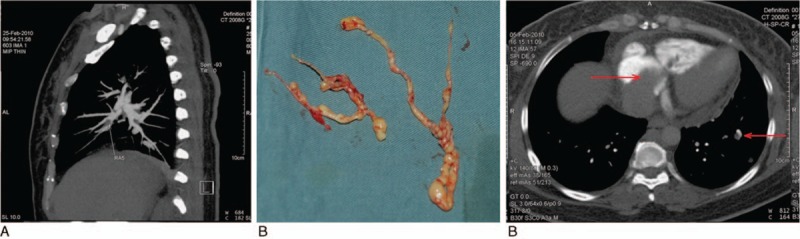
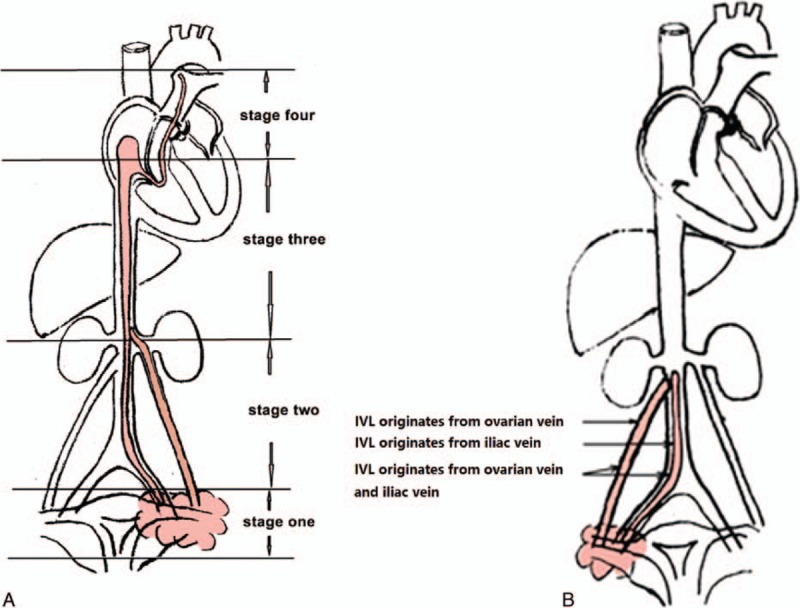
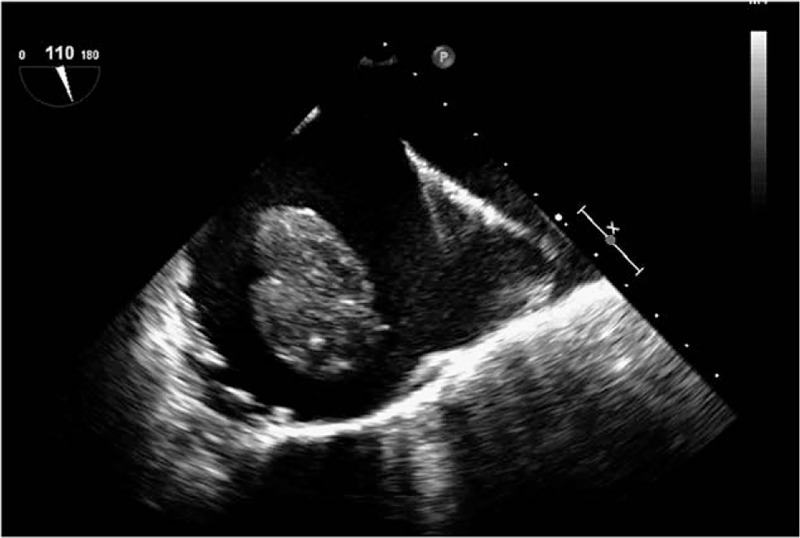
Intravenous leiomyomatosis (IVL) is a rare benign tumor. The study aimed to assess outcomes of patients treated surgically for IVL.Between November 2002 and January 2015, 76 patients were treated for IVL. The stage of IVL was evaluated preoperatively by echocardiography and enhanced computerized tomography (CT) scan, and graded into 4 stages according to intravascular tumor progression. We recorded age, lower limb edema before surgery, surgical parameters, and hospitalization expenses. Patients were followed up every 6 months and tumor recurrence was assessed by CT and ultrasound. Patients were followed up for a mean of 4.5 ± 2.5 years (range 1-13 years) and there was no operative, hospital, or long-term mortality or were lost to follow-up.The rate of lower extremity edema, amount of blood loss, postoperative transfusion, length of intensive care unit (ICU) stay, postoperative hospitalization, and hospitalization expenses differed significantly between patients at different presurgery stages. Tumors recurred in 4 of 7 patients with stage I IVL that opted for surgery that preserved the ovaries and uterus. No recurrence was observed in patients graded stage II or more, in all of which the uterus and ovaries were removed. Recurrence was observed in only 4 of 76 cases of IVL, all of whom opted for surgery that spared the ovaries and uterus.Different surgical strategies should be decided based on the staging to completely remove the tumor and ensure the safety of patients. Removal of both ovaries is necessary for inhibiting tumor growth and avoiding recurrence.
Conflict of interest statement
The authors have no conflicts of interest to disclose.
Figures
References
-
- Birch-Hirschfeld FV. Lehrbuch der pathologischen anatomie. 1896; Leipzig, Germany: FCW Vogel, 226–258.
-
- Dürck H. Ueber ein kontinvierlich durch die learned Holvene in das Herz vorwachsendes Fibromyom des Uterus. München Med Wochenschr 1907; 54:1154.
-
- Choi IJ, Han MS, Cha MS. A huge case of intravenous leiomyomatosis with intracardiac extension. J Women Med 2010; 3:29–31.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
