

Evaluation of RBC Transfusion Practice in Adult ICUs and the Effect of Restrictive Transfusion Protocols on Routine Care
- PMID: 27632673
- PMCID: PMC5547397
- DOI: 10.1097/CCM.0000000000002077
Evaluation of RBC Transfusion Practice in Adult ICUs and the Effect of Restrictive Transfusion Protocols on Routine Care
Abstract
Objective: Research supports the efficacy and safety of restrictive transfusion protocols to reduce avoidable RBC transfusions, but evidence of their effectiveness in practice is limited. This study assessed whether admission to an ICU with an restrictive transfusion protocol reduces the likelihood of transfusion for adult patients.
Design: Observational study using data from the multicenter, cohort Critical Illness Outcomes Study. Patient-level analyses were conducted with RBC transfusion on day of enrollment as the outcome and admission to an ICU with a restrictive transfusion protocol as the exposure of interest. Covariates included demographics, hospital course (e.g., lowest hematocrit, blood loss), severity of illness (e.g., Sequential Organ Failure Assessment score), interventions (e.g., sedation/analgesia), and ICU characteristics (e.g., size). Multivariable logistic regression modeling assessed the independent effects of restrictive transfusion protocols on transfusions.
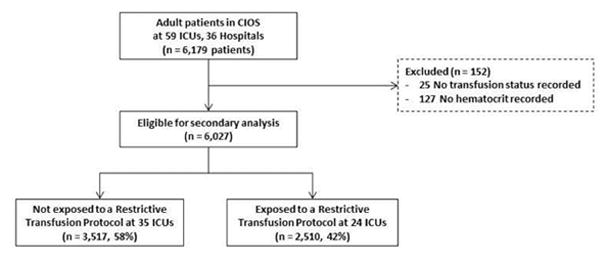
Setting: Fifty-nine U.S. ICUs.
Patients: A total of 6,027 adult ICU patients.
Interventions: None.
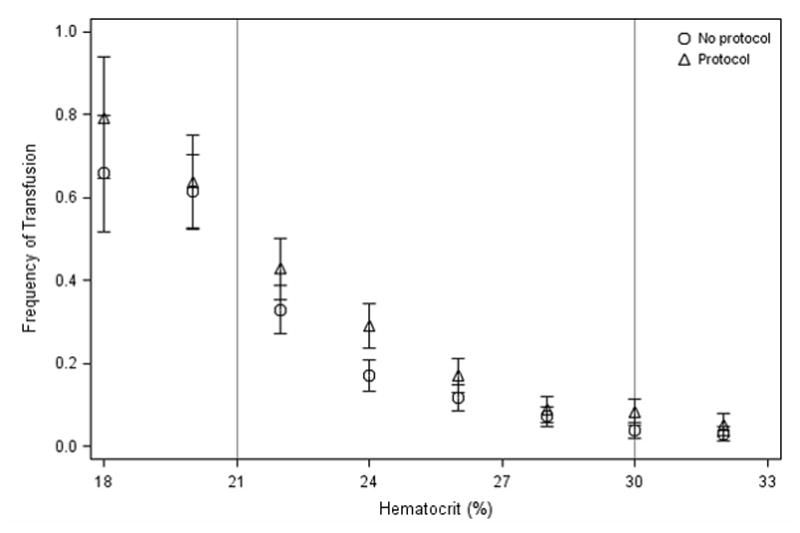
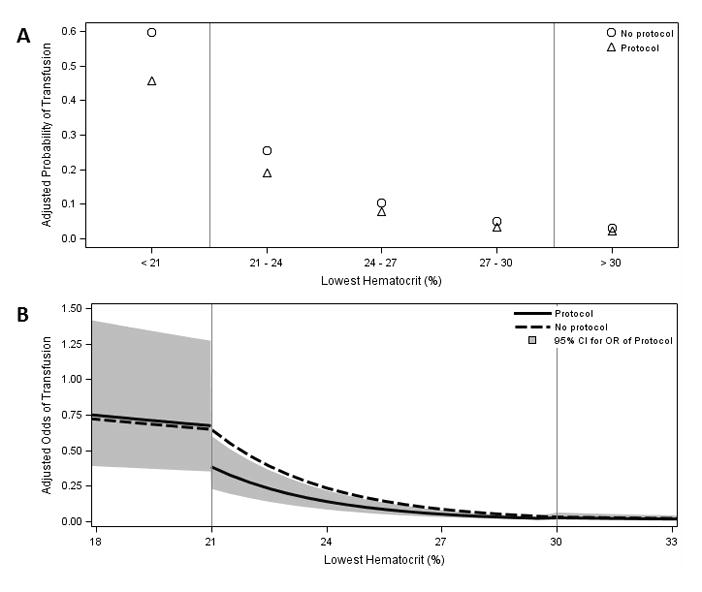
Measurements and main results: Of the 59 study ICUs, 24 had an restrictive transfusion protocol; 2,510 patients (41.6%) were in an ICU with an restrictive transfusion protocol. The frequency of RBC transfusion among patients with severe (hematocrit, < 21%), moderate (hematocrit, 21-30%), and mild (hematocrit, > 30%) anemia in restrictive transfusion protocol ICUs was 67%, 19%, and 4%, respectively, compared with 60%, 14%, and 2% for those in ICUs without an restrictive transfusion protocol. Only 27% of transfusions were associated with a hematocrit less than 21%. Adjusting for confounding factors, restrictive transfusion protocols independently reduced the odds of transfusion in moderate anemia with an odds ratio of 0.59 (95% CI, 0.36-0.96) while demonstrating no effect in mild (p = 0.93) or severe (p = 0.52) anemia.
Conclusions: In this sample of ICU patients, transfusions often occurred outside evidence-based guidelines, but admission to an ICU with an restrictive transfusion protocol did reduce the risk of transfusion in moderately anemic patients controlling for patient and ICU factors. This study supports the effectiveness of restrictive transfusion protocols for influencing transfusions in clinical practice.
Conflict of interest statement
Figures
References
-
- Vincent JL, et al. Anemia and blood transfusion in critically ill patients. JAMA. 2002;288(12):1499–507. - PubMed
-
- Corwin HL, et al. The CRIT Study: Anemia and blood transfusion in the critically ill--current clinical practice in the United States. Crit Care Med. 2004;32(1):39–52. - PubMed
-
- Nguyen BV, et al. Time course of hemoglobin concentrations in nonbleeding intensive care unit patients. Crit Care Med. 2003;31(2):406–10. - PubMed
-
- Shander A, et al. Activity-based costs of blood transfusions in surgical patients at four hospitals. Transfusion. 2010;50(4):753–65. - PubMed
-
- Marik PE, Corwin HL. Efficacy of red blood cell transfusion in the critically ill: a systematic review of the literature. Crit Care Med. 2008;36(9):2667–74. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
