

Cytokine Release Syndrome After Chimeric Antigen Receptor T Cell Therapy for Acute Lymphoblastic Leukemia
- PMID: 27632680
- PMCID: PMC5452983
- DOI: 10.1097/CCM.0000000000002053
Cytokine Release Syndrome After Chimeric Antigen Receptor T Cell Therapy for Acute Lymphoblastic Leukemia
Abstract
Objective: Initial success with chimeric antigen receptor-modified T cell therapy for relapsed/refractory acute lymphoblastic leukemia is leading to expanded use through multicenter trials. Cytokine release syndrome, the most severe toxicity, presents a novel critical illness syndrome with limited data regarding diagnosis, prognosis, and therapy. We sought to characterize the timing, severity, and intensive care management of cytokine release syndrome after chimeric antigen receptor-modified T cell therapy.
Design: Retrospective cohort study.
Setting: Academic children's hospital.
Patients: Thirty-nine subjects with relapsed/refractory acute lymphoblastic leukemia treated with chimeric antigen receptor-modified T cell therapy on a phase I/IIa clinical trial (ClinicalTrials.gov number NCT01626495).
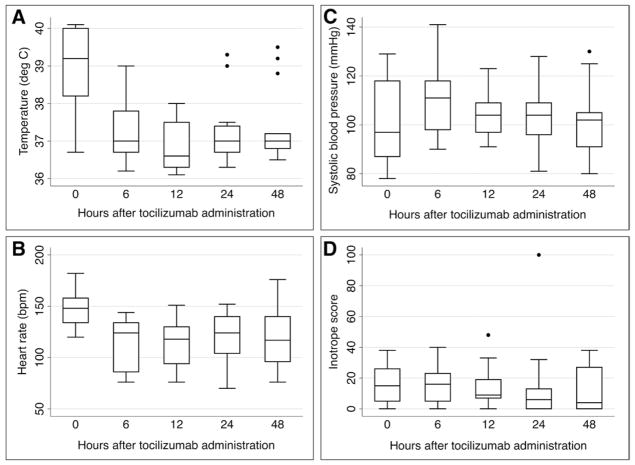
Interventions: All subjects received chimeric antigen receptor-modified T cell therapy. Thirteen subjects with cardiovascular dysfunction were treated with the interleukin-6 receptor antibody tocilizumab.
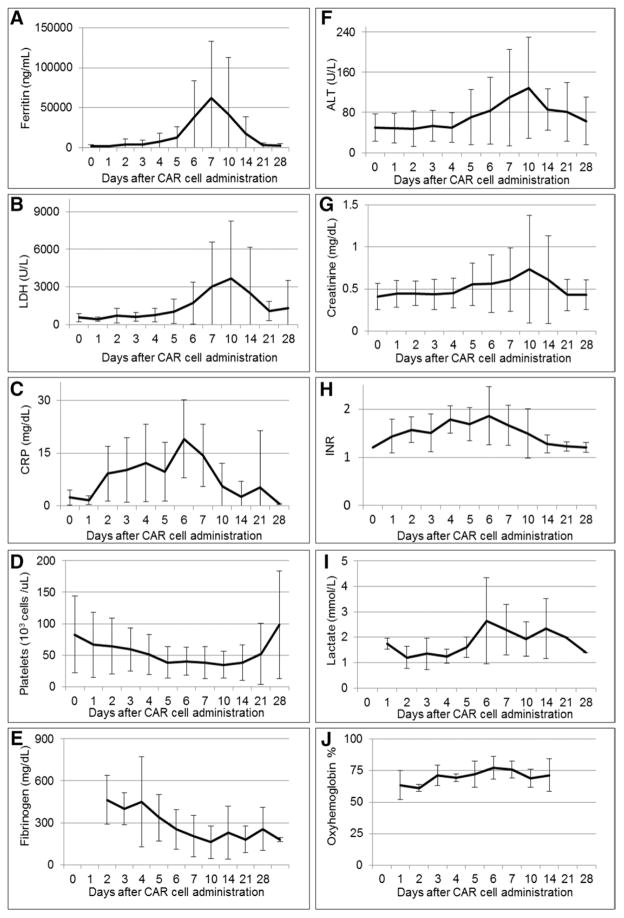
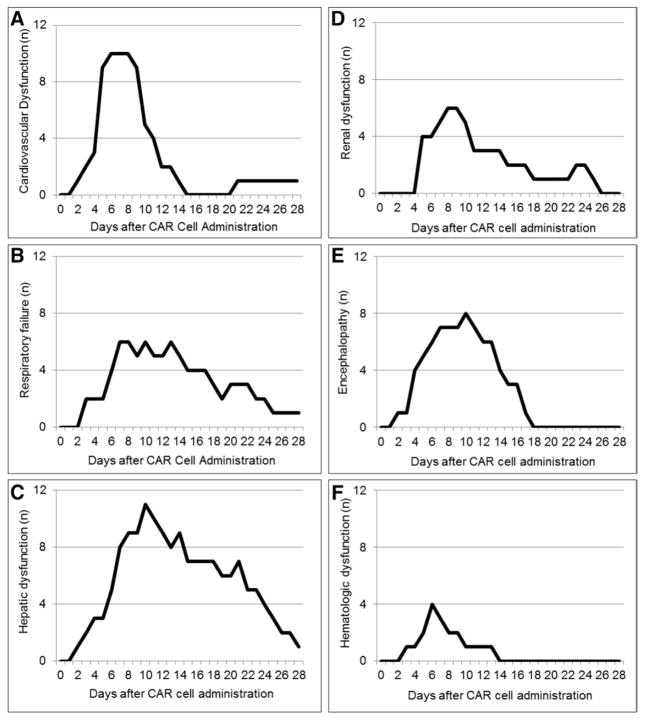
Measurements and main results: Eighteen subjects (46%) developed grade 3-4 cytokine release syndrome, with prolonged fever (median, 6.5 d), hyperferritinemia (median peak ferritin, 60,214 ng/mL), and organ dysfunction. Fourteen (36%) developed cardiovascular dysfunction treated with vasoactive infusions a median of 5 days after T cell therapy. Six (15%) developed acute respiratory failure treated with invasive mechanical ventilation a median of 6 days after T cell therapy; five met criteria for acute respiratory distress syndrome. Encephalopathy, hepatic, and renal dysfunction manifested later than cardiovascular and respiratory dysfunction. Subjects had a median of 15 organ dysfunction days (interquartile range, 8-20). Treatment with tocilizumab in 13 subjects resulted in rapid defervescence (median, 4 hr) and clinical improvement.
Conclusions: Grade 3-4 cytokine release syndrome occurred in 46% of patients following T cell therapy for relapsed/refractory acute lymphoblastic leukemia. Clinicians should be aware of expanding use of this breakthrough therapy and implications for critical care units in cancer centers.
Figures
References
-
- Ward E, DeSantis C, Robbins A, et al. Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin. 2014;64:83–103. - PubMed
-
- Bhojwani D, Pui CH. Relapsed childhood acute lymphoblastic leukaemia. Lancet Oncol. 2013;14:e205–e217. - PubMed
-
- Raetz EA, Bhatla T. Where do we stand in the treatment of relapsed acute lymphoblastic leukemia? Hematology Am Soc Hematol Educ Program. 2012;2012:129–136. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
