

Coronary Artery Aneurysms in Kawasaki Disease: Risk Factors for Progressive Disease and Adverse Cardiac Events in the US Population
- PMID: 27633390
- PMCID: PMC5079009
- DOI: 10.1161/JAHA.116.003289
Coronary Artery Aneurysms in Kawasaki Disease: Risk Factors for Progressive Disease and Adverse Cardiac Events in the US Population
Abstract
Background: The natural history of coronary artery aneurysms (CAA) after intravenous immunoglobulin (IVIG) treatment in the United States is not well described. We describe the natural history of CAA in US Kawasaki disease (KD) patients and identify factors associated with major adverse cardiac events (MACE) and CAA regression.
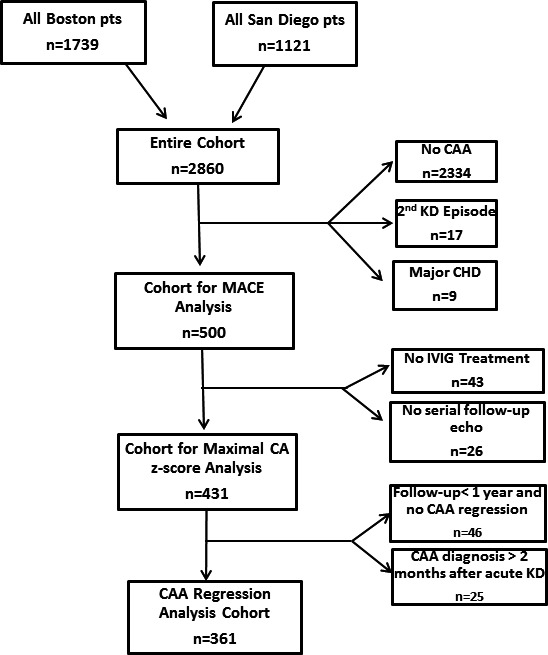
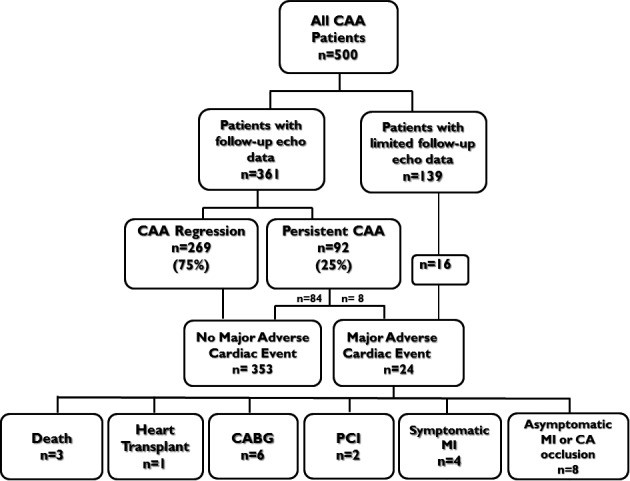
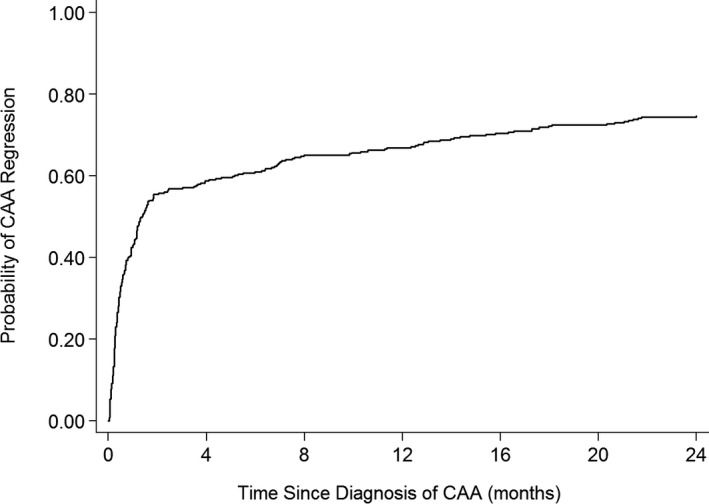
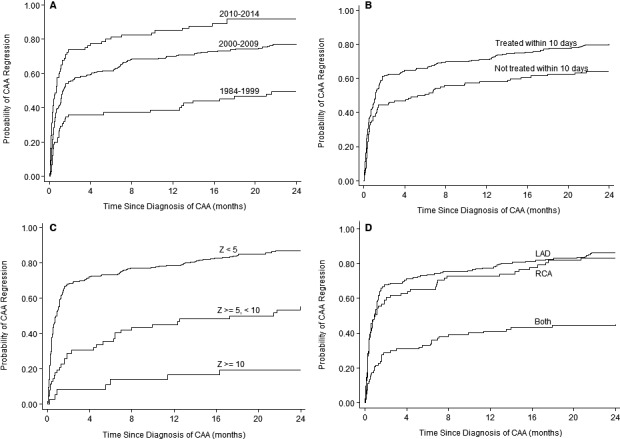
Methods and results: We evaluated all KD patients with CAA at 2 centers from 1979 to 2014. Factors associated with CAA regression, maximum CA z-score over time (zMax), and MACE were analyzed. We performed a matched analysis of treatment effect on likelihood of CAA regression. Of 2860 KD patients, 500 (17%) had CAA, including 90 with CAA z-score >10. Most (91%) received IVIG within 10 days of illness, 32% received >1 IVIG, and 27% received adjunctive anti-inflammatory medications. CAA regression occurred in 75%. Lack of CAA regression and higher CAA zMax were associated with earlier era, larger CAA z-score at diagnosis, and bilateral CAA in univariate and multivariable analyses. MACE occurred in 24 (5%) patients and was associated with higher CAA z-score at diagnosis and lack of IVIG treatment. In a subset of patients (n=132) matched by age at KD and baseline CAA z-score, those receiving IVIG plus adjunctive medication had a CAA regression rate of 91% compared with 68% for the 3 other groups (IVIG alone, IVIG ≥2 doses, or IVIG ≥2 doses plus adjunctive medication).
Conclusions: CAA regression occurred in 75% of patients. CAA z-score at diagnosis was highly predictive of outcomes, which may be improved by early IVIG treatment and adjunctive therapies.
Keywords: Kawasaki disease; cardiovascular outcomes; coronary aneurysm.
© 2016 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
References
-
- Kawasaki T. [Acute febrile mucocutaneous syndrome with lymphoid involvement with specific desquamation of the fingers and toes in children]. Arerugi. 1967;16:178–222. - PubMed
-
- Newburger JW, Takahashi M, Gerber MA, Gewitz MH, Tani LY, Burns JC, Shulman ST, Bolger AF, Ferrieri P, Baltimore RS, Wilson WR, Baddour LM, Levison ME, Pallasch TJ, Falace DA, Taubert KA; Committee on Rheumatic Fever, Endocarditis and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association . Diagnosis, treatment, and long‐term management of Kawasaki disease: a statement for health professionals from the Committee on Rheumatic Fever, Endocarditis, and Kawasaki Disease, Council on Cardiovascular Disease in the Young, American Heart Association. Pediatrics. 2004;114:1708–1733. - PubMed
-
- Burns JC, Glode MP. Kawasaki syndrome. Lancet. 2004;364:533–544. - PubMed
-
- McCrindle BW, Li JS, Minich LL, Colan SD, Atz AM, Takahashi M, Vetter VL, Gersony WM, Mitchell PD, Newburger JW; Pediatric Heart Network I . Coronary artery involvement in children with Kawasaki disease: risk factors from analysis of serial normalized measurements. Circulation. 2007;116:174–179. - PubMed
-
- Terai M, Shulman ST. Prevalence of coronary artery abnormalities in Kawasaki disease is highly dependent on gamma globulin dose but independent of salicylate dose. J Pediatr. 1997;131:888–893. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
