

The effects of superimposed tilt and lower body negative pressure on anterior and posterior cerebral circulations
- PMID: 27634108
- PMCID: PMC5027361
- DOI: 10.14814/phy2.12957
The effects of superimposed tilt and lower body negative pressure on anterior and posterior cerebral circulations
Abstract
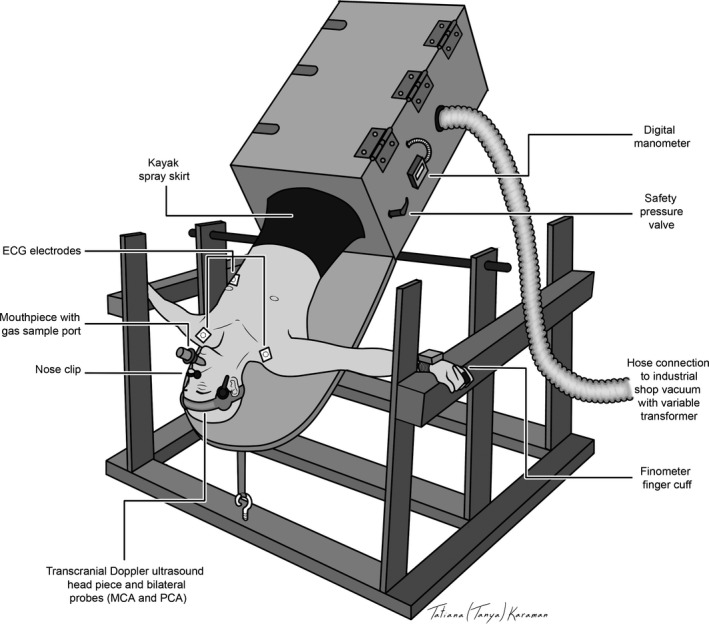
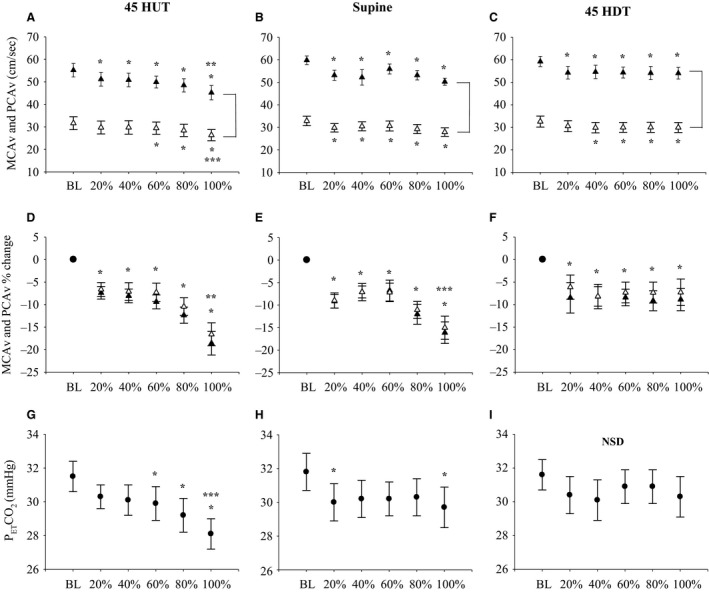
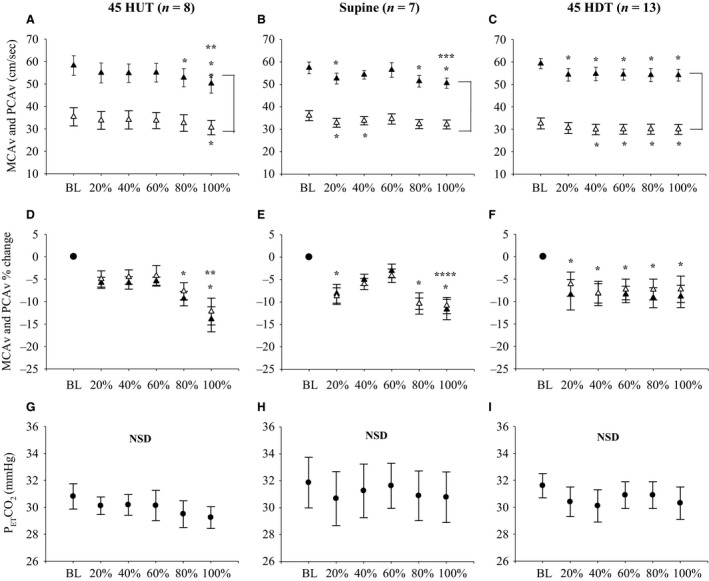
Steady-state tilt has no effect on cerebrovascular reactivity to increases in the partial pressure of end-tidal carbon dioxide (PETCO2). However, the anterior and posterior cerebral circulations may respond differently to a variety of stimuli that alter central blood volume, including lower body negative pressure (LBNP). Little is known about the superimposed effects of head-up tilt (HUT; decreased central blood volume and intracranial pressure) and head-down tilt (HDT; increased central blood volume and intracranial pressure), and LBNP on cerebral blood flow (CBF) responses. We hypothesized that (a) cerebral blood velocity (CBV; an index of CBF) responses during LBNP would not change with HUT and HDT, and (b) CBV in the anterior cerebral circulation would decrease to a greater extent compared to posterior CBV during LBNP when controlling PETCO2 In 13 male participants, we measured CBV in the anterior (middle cerebral artery, MCAv) and posterior (posterior cerebral artery, PCAv) cerebral circulations using transcranial Doppler ultrasound during LBNP stress (-50 mmHg) in three body positions (45°HUT, supine, 45°HDT). PETCO2 was measured continuously and maintained at constant levels during LBNP through coached breathing. Our main findings were that (a) steady-state tilt had no effect on CBV responses during LBNP in both the MCA (P = 0.077) and PCA (P = 0.583), and (b) despite controlling for PETCO2, both the MCAv and PCAv decreased by the same magnitude during LBNP in HUT (P = 0.348), supine (P = 0.694), and HDT (P = 0.407). Here, we demonstrate that there are no differences in anterior and posterior circulations in response to LBNP in different body positions.
Keywords: Central hypovolemia; cerebral blood velocity; head‐down tilt; head‐up tilt; lower body negative pressure.
© 2016 The Authors. Physiological Reports published by Wiley Periodicals, Inc. on behalf of the American Physiological Society and The Physiological Society.
Figures
References
-
- Aaslid, R. , Markwalder T. M., and Nornes H.. 1982. Noninvasive transcranial Doppler ultrasound recording of flow velocity in basal cerebral arteries. J. Neurosurg. 57:769–774. - PubMed
-
- Ainslie, P. N. , and Duffin J.. 2009. Integration of cerebrovascular CO2 reactivity and chemoreflex control of breathing: mechanisms of regulation, measurement, and interpretation. Am. J. Physiol. Regul. Integr. Comp. Physiol. 296:R1473–95. - PubMed
-
- Ainslie, P. N. , and Hoiland R. L.. 2014. Transcranial Doppler ultrasound: valid, invalid, or both? J. Appl. Physiol.(1985) 117: 1081–1083. - PubMed
-
- Bain, A. R. , Smith K. J., Lewis N. C., Foster G. E., Wildfong K. W., Willie C. K., et al. 2013. Regional changes in brain blood flow during severe passive hyperthermia: effects of PaCO2 and extracranial blood flow. J. Appl. Physiol. 115:653–9. - PubMed
-
- Brown, C. M. , Dutsch M., Hecht M. J., Neundorfer B., and Hilz M. J.. 2003. Assessment of cerebrovascular and cardiovascular responses to lower body negative pressure as a test of cerebral autoregulation. J. Neurol. Sci. 208(1–2):71–78. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
