

Subnational variation for care at birth in Tanzania: is this explained by place, people, money or drugs?
- PMID: 27634353
- PMCID: PMC5025821
- DOI: 10.1186/s12889-016-3404-3
Subnational variation for care at birth in Tanzania: is this explained by place, people, money or drugs?
Abstract
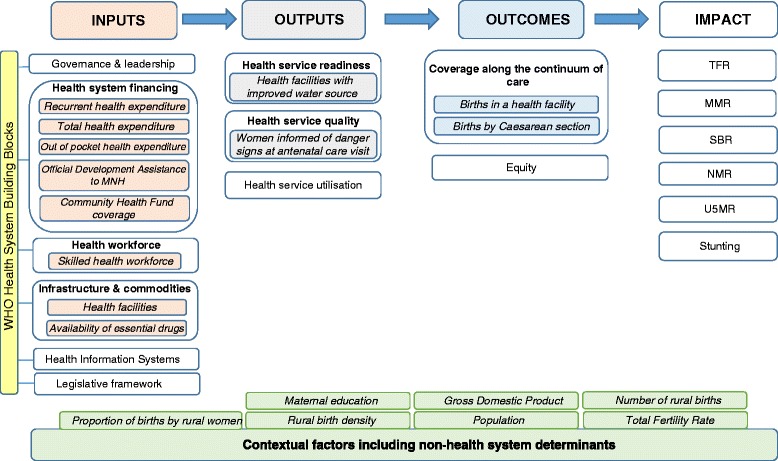
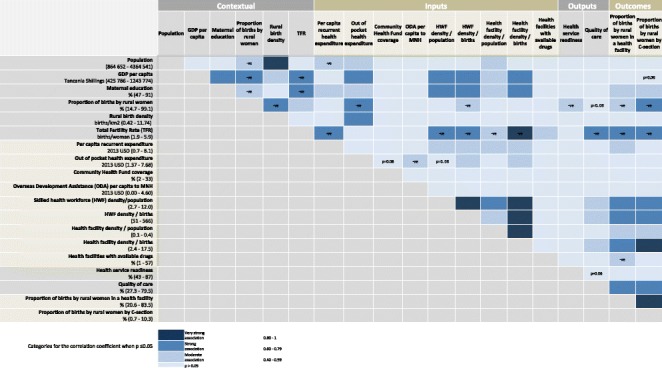
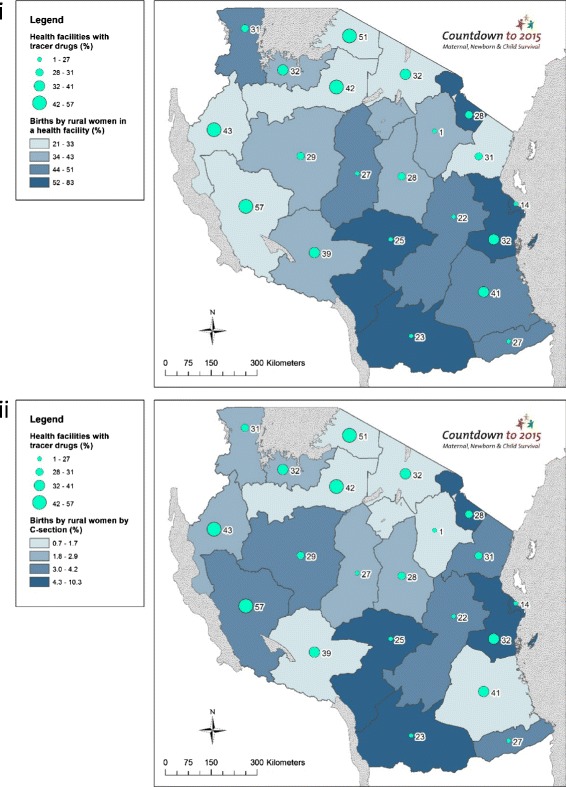
Background: Tanzania achieved the Millennium Development Goal for child survival, yet made insufficient progress for maternal and neonatal survival and stillbirths, due to low coverage and quality of services for care at birth, with rural women left behind. Our study aimed to evaluate Tanzania's subnational (regional-level) variations for rural care at birth outcomes, i.e., rural women giving birth in a facility and by Caesarean section (C-section), and associations with health systems inputs (financing, health workforce, facilities, and commodities), outputs (readiness and quality of care) and context (education and GDP).
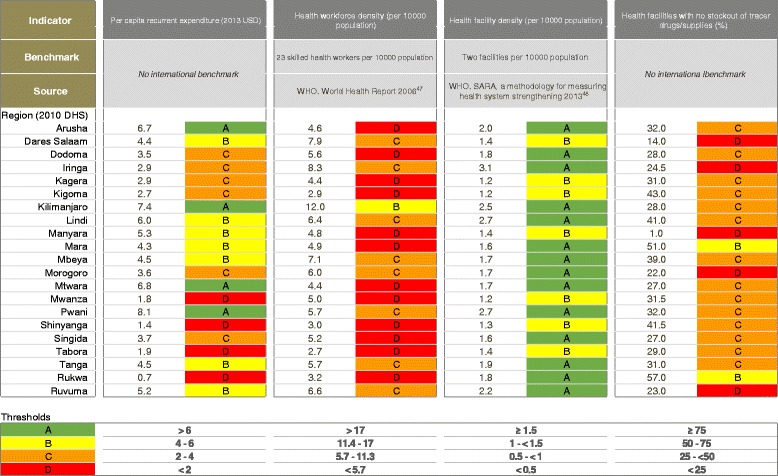
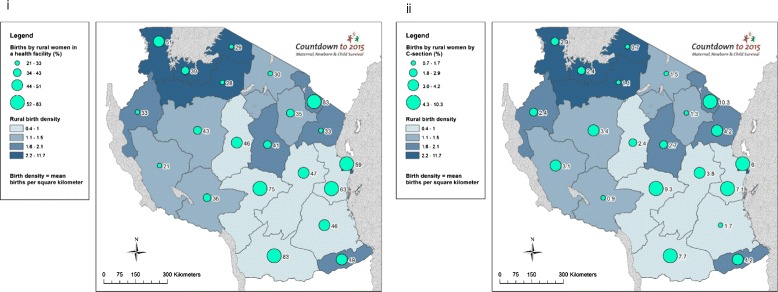
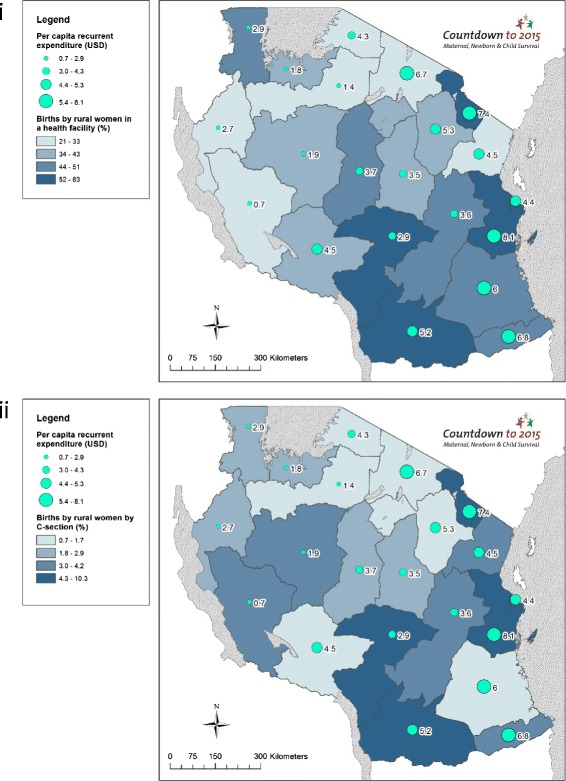
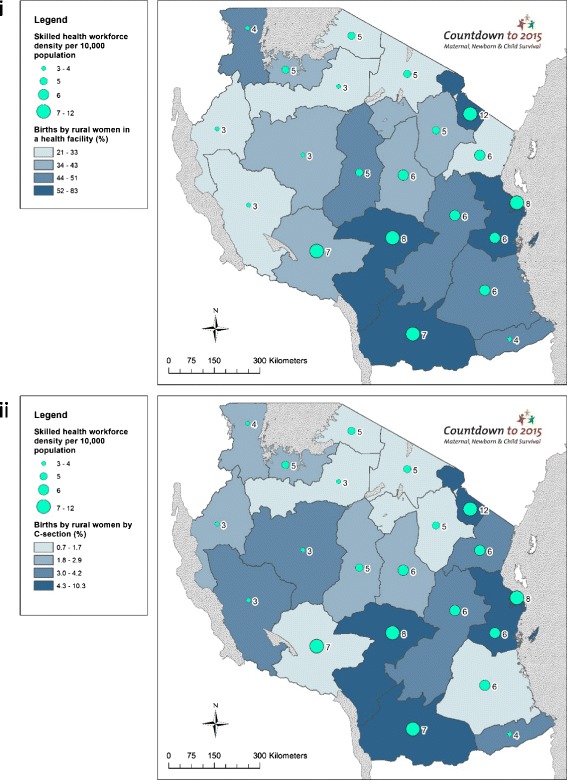
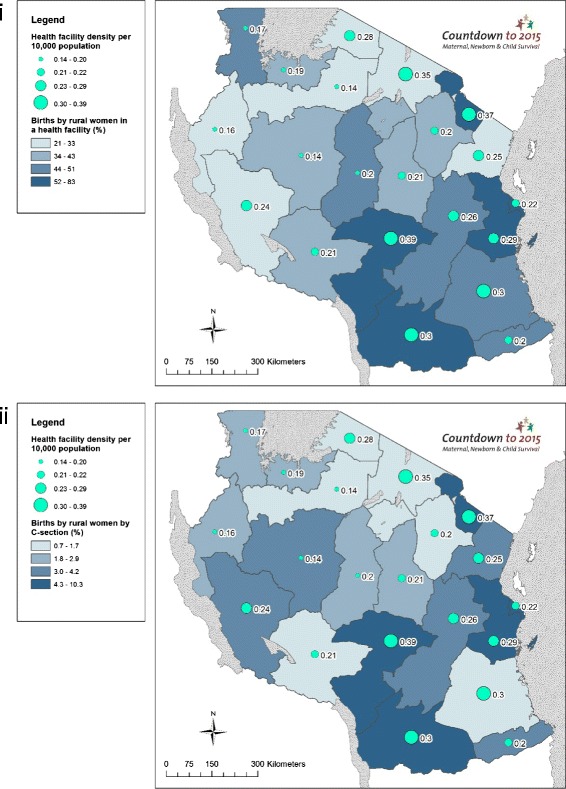
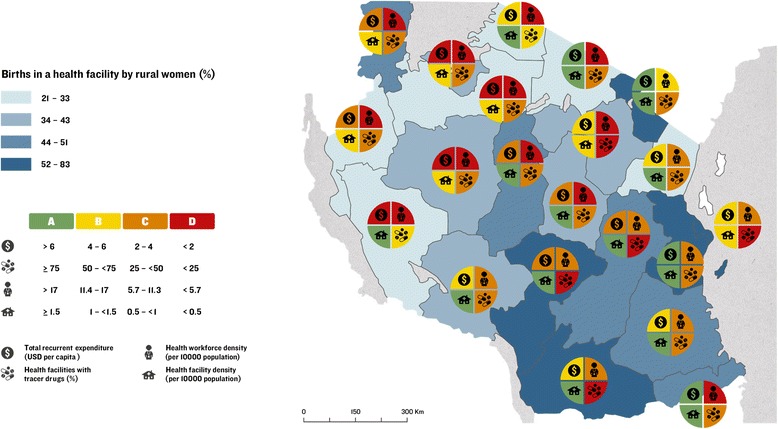
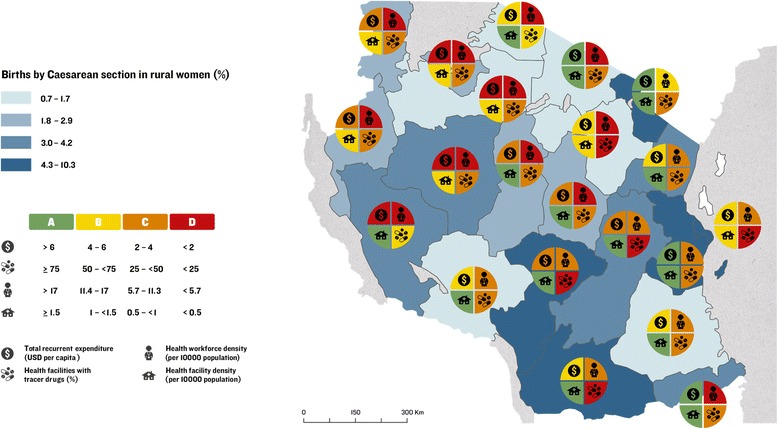
Methods: We undertook correlation analyses of subnational-level associations between health system inputs, outputs, context, and rural care at birth outcomes; and constructed implementation readiness barometers using benchmarks for each health system input indicator. We used geographical information system (GIS) mapping to visualise subnational variations in care at birth for rural women, with a focus on service availability and readiness, and collected qualitative data to investigate financial flows from national to council level to understand variation in financing inputs.
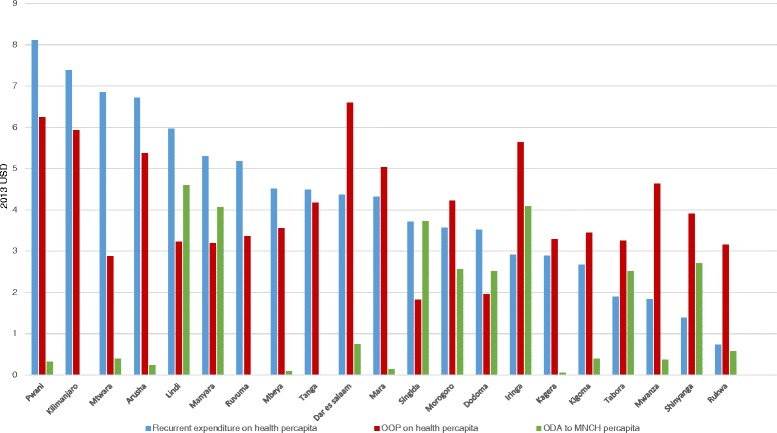
Results: We found wide subnational variation for rural care at birth outcomes, health systems inputs, and contextual indicators. There was a positive association between rural women giving birth in a facility and by C-section; maternal education; workforce and facility density; and quality of care. There was a negative association between these outcomes and proportion of all births to rural women, total fertility rate, and availability of essential commodities at facilities. Per capita recurrent expenditure was positively associated with facility births (correlation coefficient = 0.43; p = 0.05) but not with C-section. Qualitative results showed that the health financing system is complex and insufficient for providing care at birth services. Bottlenecks for care at birth included low density of health workers, poor availability of essential commodities, and low health financing in Lake and Western Zones.
Conclusions: No region meets the benchmarks for the four health systems building blocks including health finance, health workforce, health facilities, and commodities. Strategies for addressing health system inequities, including overall increases in health expenditure, are needed in rural populations and areas of highest unmet need for family planning to improve coverage of care at birth for rural women in Tanzania.
Keywords: Childbirth; Health financing; Health systems; Health workforce; Maternal health; Newborn health; Quality of care; Tanzania.
Figures
References
-
- UNICEF, UN Inter-agency Group for Child Mortality Estimation. Levels and Trends in Child Mortality 2015: Estimates Developed by the UN Inter-agency Group for Child Mortality Estimation. New York: UNICEF; 2015.
-
- WHO, UNICEF, UNFPA, The World Bank . Trends in Maternal Mortality: 1990 to 2015. Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division Geneva. 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
