

Effect of abdominopelvic abscess drain size on drainage time and probability of occlusion
- PMID: 27634422
- PMCID: PMC5315689
- DOI: 10.1016/j.amjsurg.2016.07.027
Effect of abdominopelvic abscess drain size on drainage time and probability of occlusion
Abstract
Background: The purpose of this study is to determine whether larger abdominopelvic abscess drains reduce the time required for abscess resolution or the probability of tube occlusion.
Methods: 144 consecutive patients who underwent abscess drainage at a single institution were reviewed retrospectively.
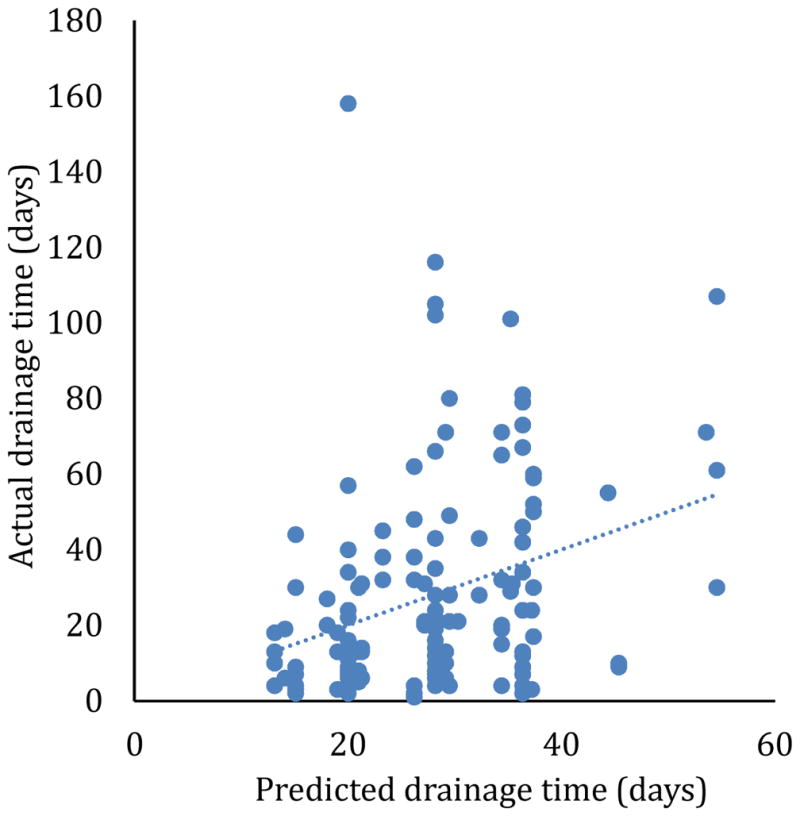
Results: Larger initial drain size did not reduce drainage time, drain occlusion, or drain exchanges (P > .05). Subgroup analysis did not find any type of collection that benefitted from larger drains. A multivariate model predicting drainage time showed that large collections (>200 mL) required 16 days longer drainage time than small collections (<50 mL). Collections with a fistula to bowel required 17 days longer drainage time than collections without a fistula. Initial drain size and the viscosity of the fluid in the collection had no significant effect on drainage time in the multivariate model.
Conclusions: 8 F drains are adequate for initial drainage of most serous and serosanguineous collections. 10 F drains are adequate for initial drainage of most purulent or bloody collections.
Keywords: Abscess; Drainage; Fistula.
Copyright © 2016 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
References
-
- Gerzof SG, Robbins AH, Birkett DH. Computed tomography in the diagnosis and management of abdominal abscesses. Gastrointestinal Radiology. 1978;3(1):287–94. - PubMed
-
- vanSonnenberg E, Wittich GR, Goodacre BW, et al. Percutaneous abscess drainage: update. World J Surg. 2001 Mar;25(3):362–9. discussion 70-2. Epub 2001/05/09. eng. - PubMed
-
- Robert B, Yzet T, Regimbeau JM. Radiologic drainage of post-operative collections and abscesses. J Visc Surg. 2013 Jun;150(3 Suppl):S11–8. Epub 2013/06/25. eng. - PubMed
-
- Gee MS, Kim JY, Gervais DA, et al. Management of abdominal and pelvic abscesses that persist despite satisfactory percutaneous drainage catheter placement. AJR Am J Roentgenol. 2010 Mar;194(3):815–20. Epub 2010/02/23. eng. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
