

Intravascular large B-cell lymphoma associated with silicone breast implant, HLA-DRB1*11:01, and HLA-DQB1*03:01 manifesting as macrophage activation syndrome and with severe neurological symptoms: a case report
- PMID: 27634631
- PMCID: PMC5025582
- DOI: 10.1186/s13256-016-0993-5
Intravascular large B-cell lymphoma associated with silicone breast implant, HLA-DRB1*11:01, and HLA-DQB1*03:01 manifesting as macrophage activation syndrome and with severe neurological symptoms: a case report
Abstract
Background: Silicone implants have been successfully used for breast augmentation and reconstruction in millions of women worldwide. The reaction to the silicone implant is highly variable; it can lead to local inflammatory symptoms, and sometimes to systemic symptoms and disease. Over 80 cases of anaplastic lymphoma kinase-negative anaplastic large cell lymphoma have been reported in patients with silicone breast implants and have been accepted as a new clinical entity. To the best of our knowledge, an intravascular large B-cell lymphoma associated with a silicone breast implant has not been reported previously.
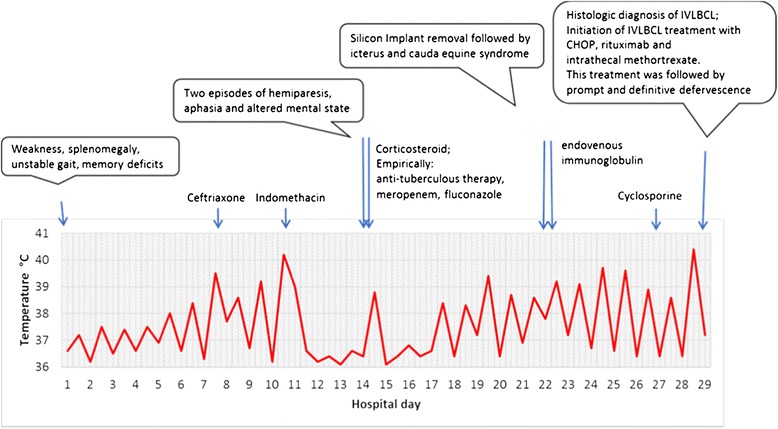
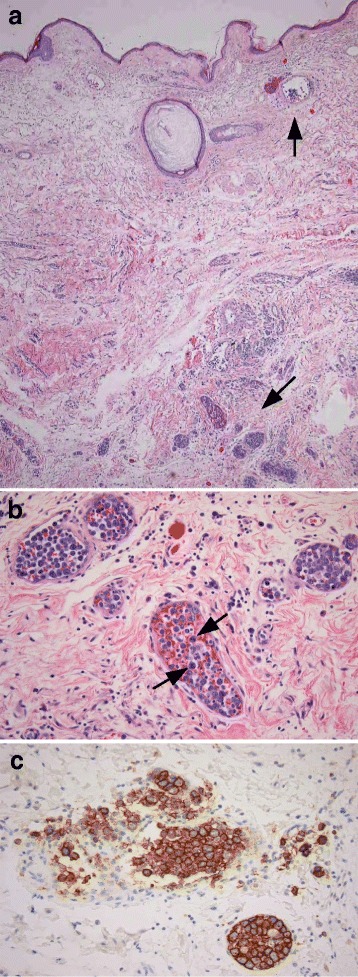
Case presentation: A 48-year-old Caucasian woman who presented with high fever was found to have splenomegaly on physical examination. A laboratory diagnosis revealed pancytopenia, hypertriglyceridemia, and hyperferritinemia. She developed signs of altered sensorium, hemiparesis, aphasia, and cauda equina syndrome. On further evaluation, she fulfilled the necessary five out of eight criteria for diagnosis of macrophage activation syndrome/hemophagocytic lymphohistiocytosis. Dexamethasone administration was followed by prompt improvement; however, 3 days later she again manifested high fever, which persisted despite administration of immunoglobulin and cyclosporine A. Her silicone breast implant was considered a possible contributor to her macrophage activation syndrome and was therefore removed. A histological examination of the capsule tissue showed an extensive lymphohistiocytic/giant cell foreign body reaction suggestive of autoimmune/inflammatory syndrome induced by adjuvants. However, the histological examination unexpectedly also revealed an intravascular large B-cell lymphoma.
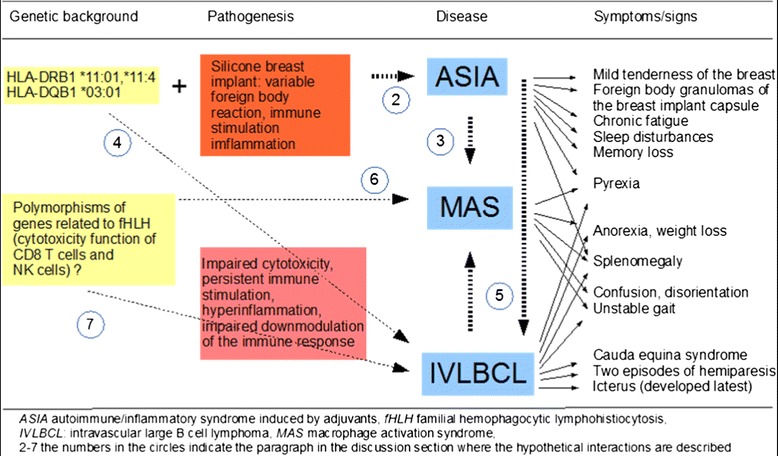
Conclusions: The genetic background of our patient with silicone breast implants might have predisposed her to three rare and difficult to diagnose syndromes/diseases: macrophage activation syndrome/hemophagocytic lymphohistiocytosis, autoimmune/inflammatory syndrome induced by adjuvants, and intravascular large B-cell lymphoma. The simultaneous manifestation of all three syndromes suggests causal interrelationships. Human leukocyte antigen testing in all women who undergo silicon breast implantation could in the future enable us to better evaluate the risk of potential side effects.
Keywords: Autoimmune inflammatory syndrome induced by adjuvants (ASIA); Hemophagocytic lymphohistiocytosis (HLH); Intravascular large B-cell lymphoma (IVLBCL); Macrophage activation syndrome (MAS); Silicone breast implant; Siliconosis.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
