

High-intensity meropenem combinations with polymyxin B: new strategies to overcome carbapenem resistance in Acinetobacter baumannii
- PMID: 27634916
- PMCID: PMC5161044
- DOI: 10.1093/jac/dkw355
High-intensity meropenem combinations with polymyxin B: new strategies to overcome carbapenem resistance in Acinetobacter baumannii
Abstract
Objectives: The pharmacodynamics of polymyxin/carbapenem combinations against carbapenem-resistant Acinetobacter baumannii (CRAB) are largely unknown. Our objective was to determine whether intensified meropenem regimens in combination with polymyxin B enhance killing and resistance suppression of CRAB.
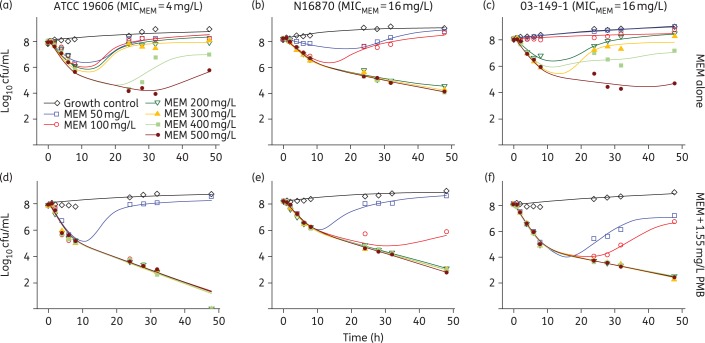
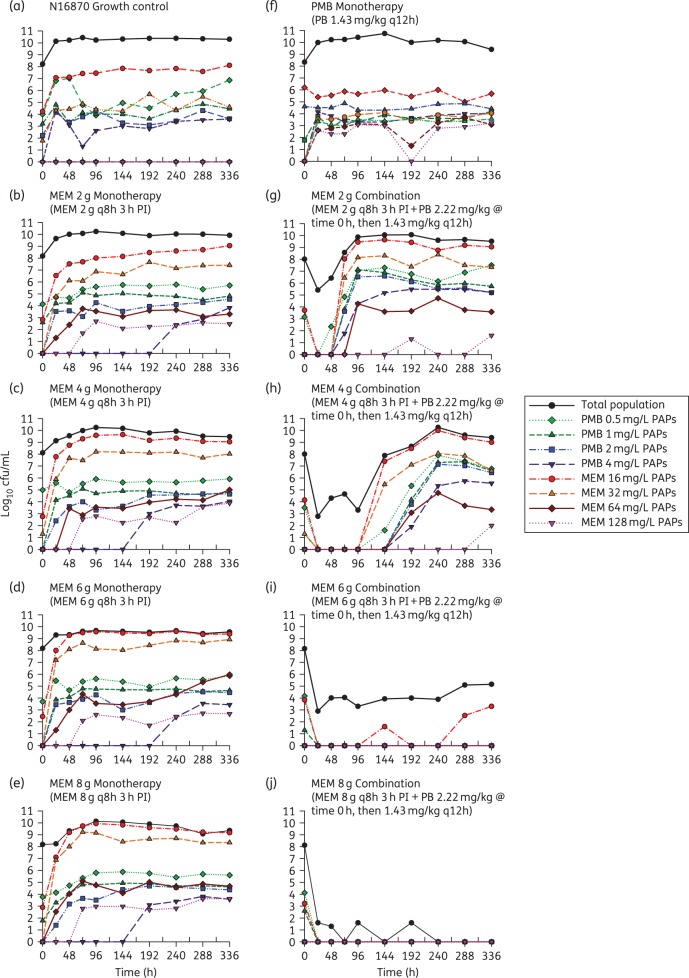
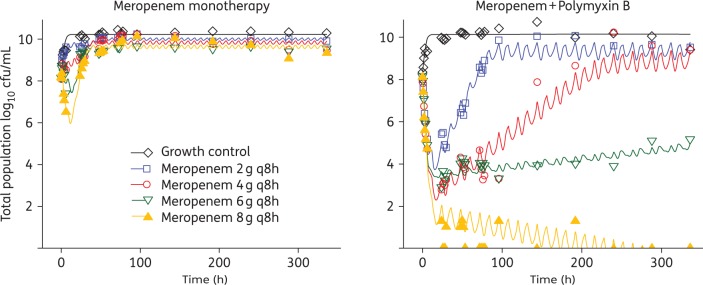
Methods: Time-kill experiments for meropenem and polymyxin B combinations were conducted against three polymyxin B-susceptible (MIC of polymyxin B = 0.5 mg/L) CRAB strains with varying meropenem MICs (ATCC 19606, N16870 and 03-149-1; MIC of meropenem = 4, 16 and 64 mg/L, respectively) at 108 cfu/mL. A hollow-fibre infection model was then used to simulate humanized regimens of polymyxin B and meropenem (2, 4, 6 and 8 g prolonged infusions every 8 h) versus N16870 at 108 cfu/mL over 14 days. New mathematical mechanism-based models were developed using S-ADAPT.
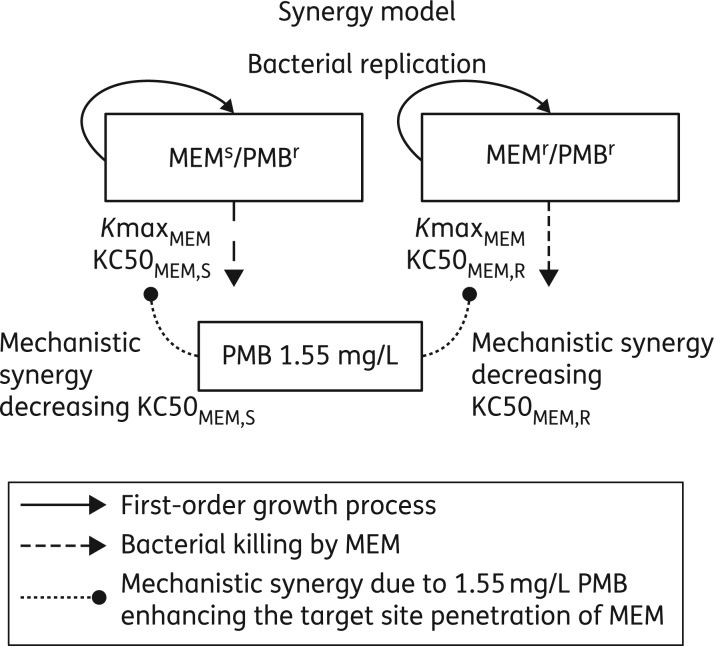
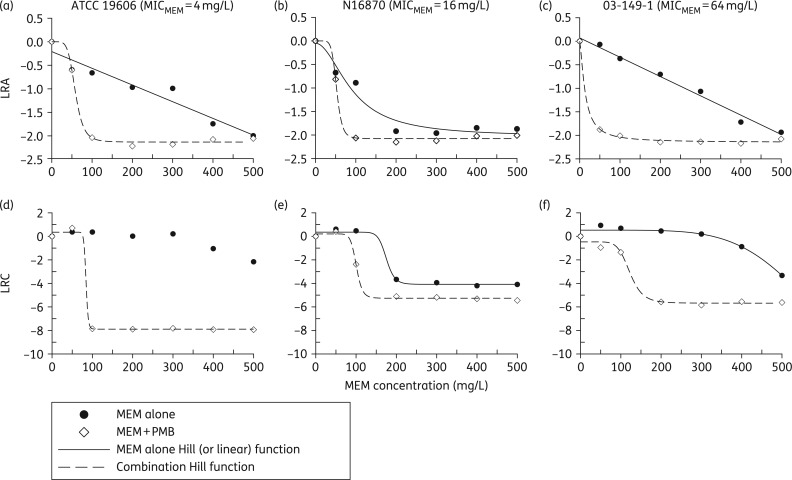
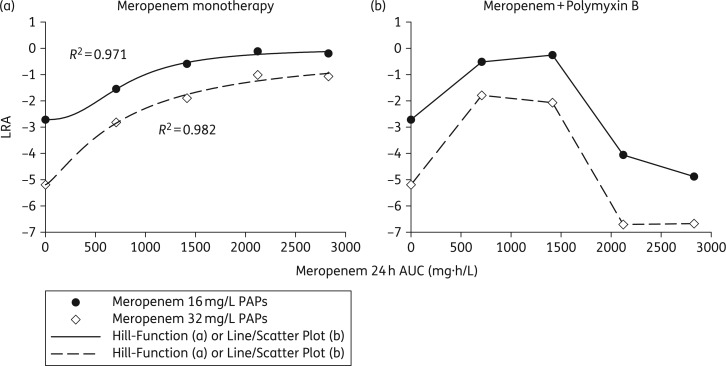
Results: Time-kill experiments were well described by the mathematical mechanism-based models, with the presence of polymyxin B drastically decreasing the meropenem concentration needed for half-maximal activity against meropenem-resistant populations from 438 to 82.1 (ATCC 19606), 158 to 93.6 (N16870) and 433 to 76.0 mg/L (03-149-1). The maximum killing effect of combination treatment was similar among all three strains despite divergent meropenem MIC values (Emax = 2.13, 2.08 and 2.15; MIC of meropenem = 4, 16 and 64 mg/L, respectively). Escalating the dose of meropenem in hollow-fibre combination regimens from 2 g every 8 h to 8 g every 8 h resulted in killing that progressed from a >2.5 log10 cfu/mL reduction with regrowth by 72 h (2 g every 8 h) to complete eradication by 336 h (8 g every 8 h).
Conclusion: Intensified meropenem dosing in combination with polymyxin B may offer a unique strategy to kill CRAB irrespective of the meropenem MIC.
© The Author 2016. Published by Oxford University Press on behalf of the British Society for Antimicrobial Chemotherapy. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures

References
-
- El-Saed A, Balkhy HH, Al-Dorzi HM et al. . Acinetobacter is the most common pathogen associated with late-onset and recurrent ventilator-associated pneumonia in an adult intensive care unit in Saudi Arabia. Int J Infect Dis 2013; 17: e696–701. - PubMed
-
- Walkey AJ, Reardon CC, Sulis CA et al. . Epidemiology of ventilator-associated pneumonia in a long-term acute care hospital. Infect Control Hosp Epidemiol 2009; 30: 319–24. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Molecular Biology Databases
