

Comparing clinical presentations, treatments and outcomes of hepatocellular carcinoma due to hepatitis C and non-alcoholic fatty liver disease
- PMID: 27634970
- PMCID: PMC5444673
- DOI: 10.1093/qjmed/hcw151
Comparing clinical presentations, treatments and outcomes of hepatocellular carcinoma due to hepatitis C and non-alcoholic fatty liver disease
Abstract
Introduction: Hepatocellular carcinoma (HCC) is increasing in incidence in the UK and globally. Liver cirrhosis is the common cause for developing HCC. The common reasons for liver cirrhosis are viral hepatitis C (HCV), viral hepatitis B and alcohol. However, HCC caused by non-alcoholic fatty liver disease (NAFLD)-cirrhosis is now increasingly as a result of rising worldwide obesity.
Aim: : To compare the clinical presentation, treatment options and outcomes of HCC due to HCV and NAFLD patients.
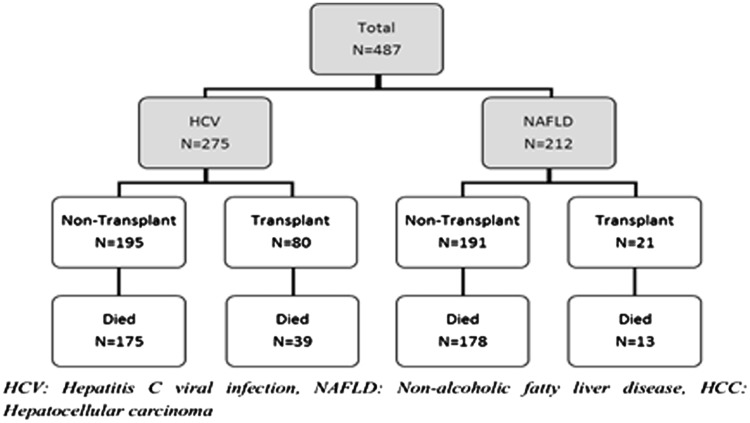
Methods: Data were collected from two liver transplant centres in the UK (Birmingham and Newcastle upon Tyne) between 2000 and 2014. We compared 275 patients with HCV-related HCC against 212 patients with NAFLD- related HCC.
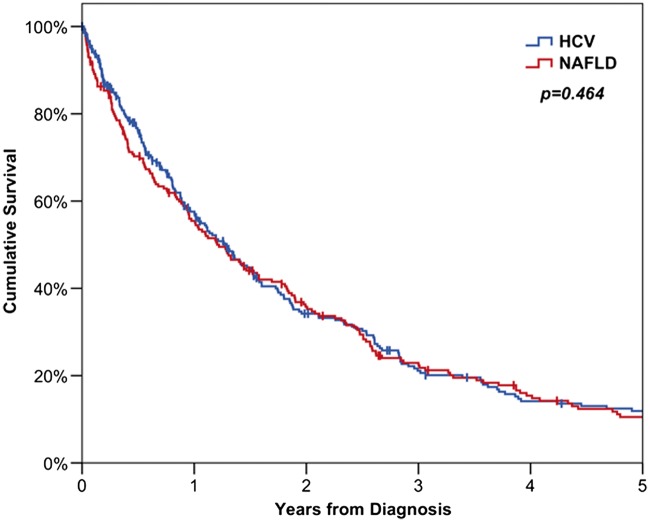
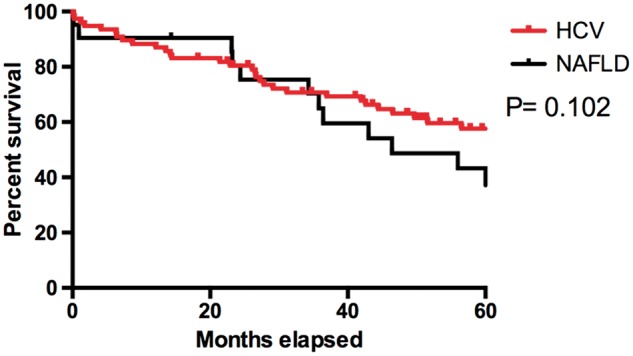
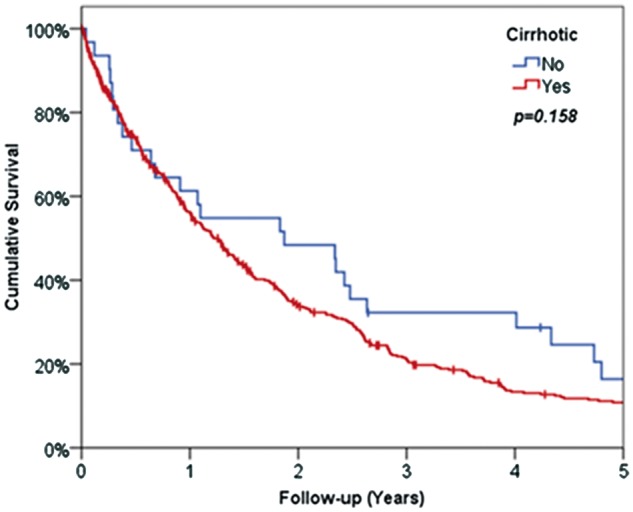
Results: Patients in the NAFLD group were found to be significantly older ( P < 0.001) and more likely to be Caucasian ( P < 0.001). They had lower rates of cirrhosis ( P < 0.001) than those in HCV-HCC group. The NAFLD group presented with significantly larger tumours ( P = 0.009), whilst HCV patients had a higher alpha fetoprotein ( P = 0.018). NAFLD patients were more commonly treated with TACE ( P = 0.005) than the HCV patients, whilst the HCV group were significantly more likely to be transplanted ( P < 0.001). In patients selected for liver transplantation, 5-year survival rates in NAFLD were not significantly different from HCV-HCC (44 and 56% respectively, P = 0.102).
Conclusion: In this study, NAFLD patients presented with larger tumours that were less likely to be amenable to curative therapy, as compared with HCV patients. Despite this disadvantage, patients with NAFLD had similar overall survival compared to patients with HCV.
© The Author 2016. Published by Oxford University Press on behalf of the Association of Physicians.
Figures
References
-
- Blachier M, Leleu H, Peck-Radosavljevic M, Valla DC, Roudot-Thoraval F. The burden of liver disease in Europe: a review of available epidemiological data. J Hepatol 2013; 58:593–608. - PubMed
-
- El-Serag HB, Mason AC. Rising incidence of hepatocellular carcinoma in the United States. N Engl J Med 1999; 340:745–50. - PubMed
-
- El-Serag HB, Rudolph KL. Hepatocellular carcinoma: epidemiology and molecular carcinogenesis. Gastroenterology 2007; 132:2557–76. - PubMed
-
- Angulo P. Nonalcoholic fatty liver disease. N Engl J Med 2002; 346:1221–31. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
