

Recovery after Acute Kidney Injury
- PMID: 27635668
- PMCID: PMC5363967
- DOI: 10.1164/rccm.201604-0799OC
Recovery after Acute Kidney Injury
Abstract
Rationale: Little is known about how acute kidney injury (AKI) resolves, and whether patterns of reversal of renal dysfunction differ among patients with respect to ultimate recovery.
Objectives: We sought to examine different patterns for AKI reversal that are found in patients and assess how they relate to postdischarge outcomes.
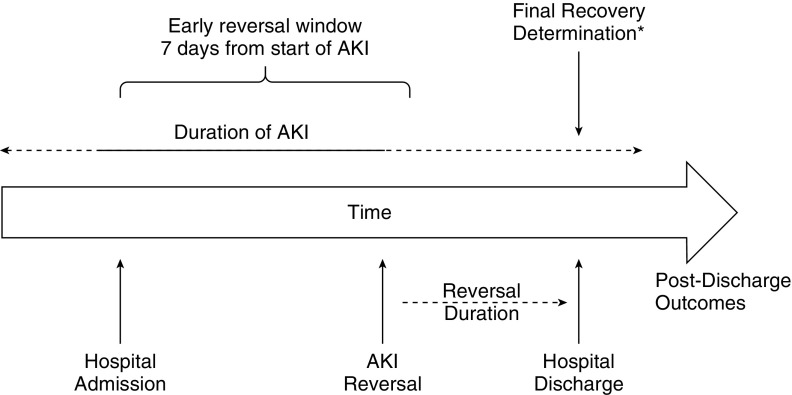
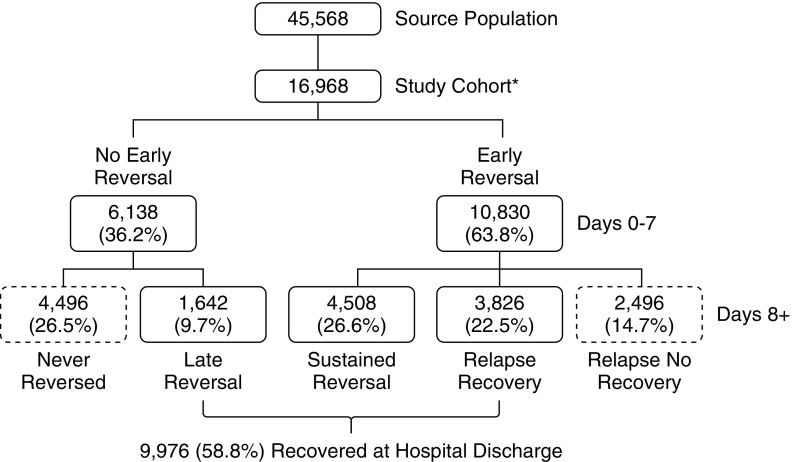
Methods: We studied 16,968 critically ill patients with Kidney Disease Improving Global Outcomes stage 2 or 3 AKI, using an electronic database. Reversal of AKI was defined as alive and no longer meeting criteria for even stage 1. Recovery was defined as reversal at hospital discharge.
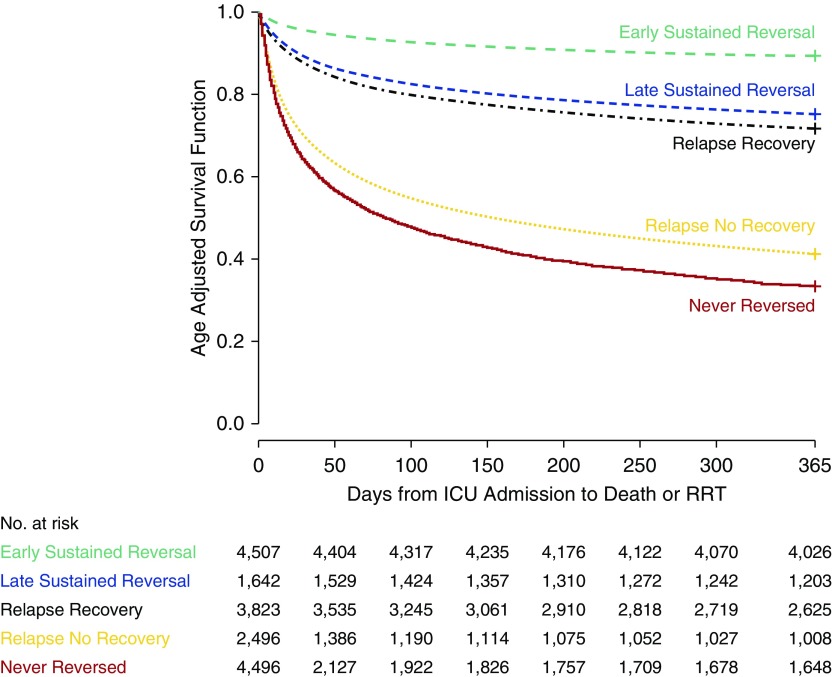
Measurements and main results: We observed five patterns. The most common (4,508; 26.6%) was early reversal that was sustained through discharge, but almost as many patients (4,496; 26.5%) had no reversal at all. The remaining patients had late reversal after Day 7 (9.7%); early reversal with one or more relapses, but with ultimate recovery (22.5%); and relapsing without recovery (14.7%). Outcomes for patients with these phenotypes were quite different, with age-adjusted 1-year survival varying from more than 90% for early reversal to less than 40% for patients never reversing. Relapses are common (37.3%), especially in the first 72 hours after reversal, and are associated with a fivefold increased risk for death by 1 year compared with early sustained reversal.
Conclusions: We have identified five distinct recovery phenotypes on the basis of the clinical course over the first week after AKI manifestation. These phenotypes may identify patients amenable to therapeutic intervention. Long-term outcomes are associated with recovery status at hospital discharge.
Keywords: critical care; dialysis; outcomes; renal failure; survival.
Figures
Comment in
-
Recovery after Acute Kidney Injury: A New Prognostic Dimension of the Syndrome.Am J Respir Crit Care Med. 2017 Mar 15;195(6):711-714. doi: 10.1164/rccm.201610-1971ED. Am J Respir Crit Care Med. 2017. PMID: 28294655 No abstract available.
References
-
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P Acute Dialysis Quality Initiative workgroup. Acute renal failure - definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group. Crit Care. 2004;8:R204–R212. - PMC - PubMed
-
- Akcan-Arikan A, Zappitelli M, Loftis LL, Washburn KK, Jefferson LS, Goldstein SL. Modified RIFLE criteria in critically ill children with acute kidney injury. Kidney Int. 2007;71:1028–1035. - PubMed
-
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury. Kidney Int Suppl. 2012;2:1–138.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
