

Fast imaging employing steady-state acquisition (FIESTA) MRI to investigate cerebrospinal fluid (CSF) within dural reflections of posterior fossa cranial nerves
- PMID: 27636022
- PMCID: PMC5124841
- DOI: 10.1259/bjr.20160392
Fast imaging employing steady-state acquisition (FIESTA) MRI to investigate cerebrospinal fluid (CSF) within dural reflections of posterior fossa cranial nerves
Abstract
Objective: There is no consensus approach to covering skull base meningeal reflections-and cerebrospinal fluid (CSF) therein-of the posterior fossa cranial nerves (CNs VII-XII) when planning radiotherapy (RT) for medulloblastoma and ependymoma. We sought to determine whether MRI and specifically fast imaging employing steady-state acquisition (FIESTA) sequences can answer this anatomical question and guide RT planning.
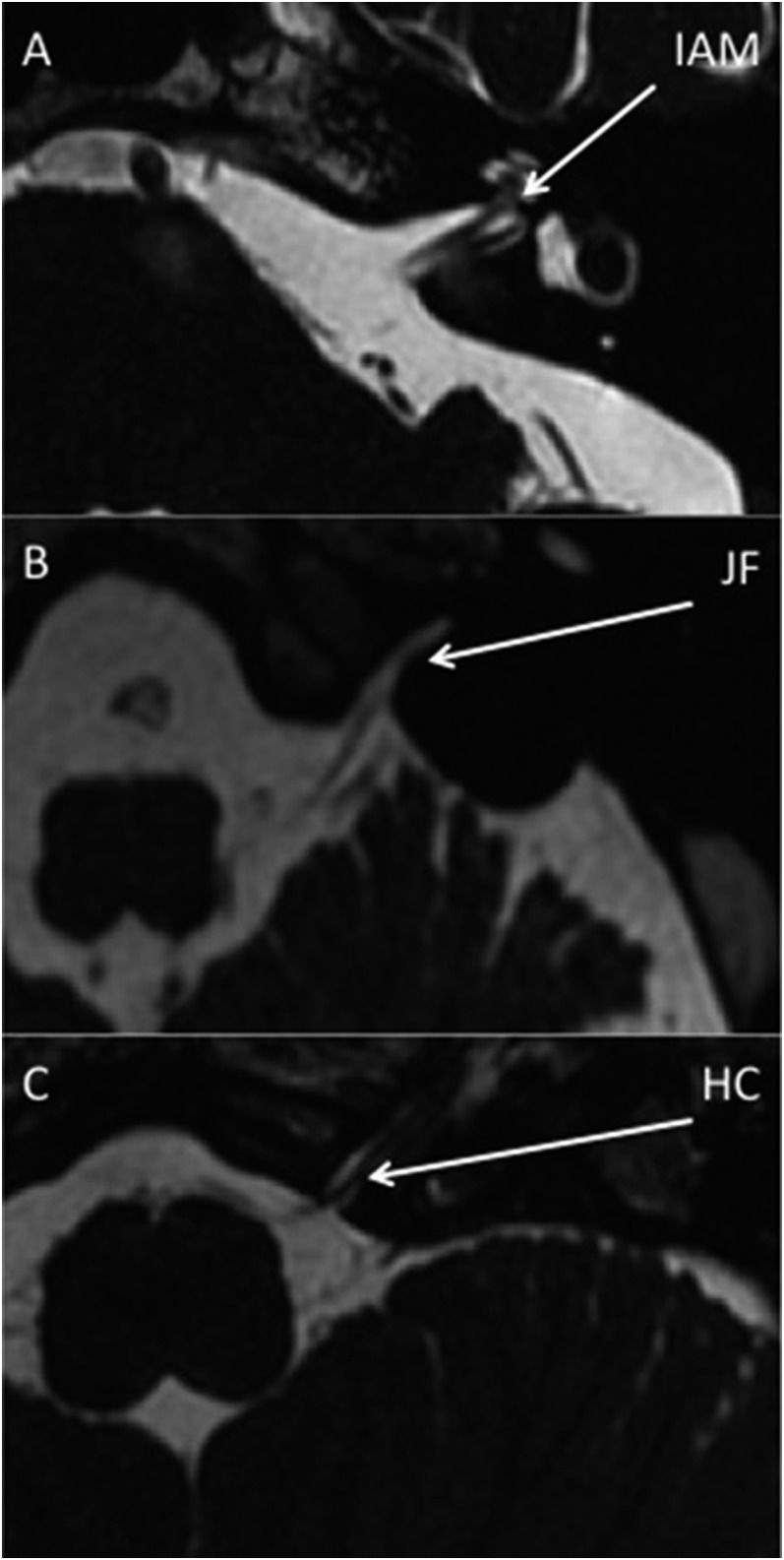
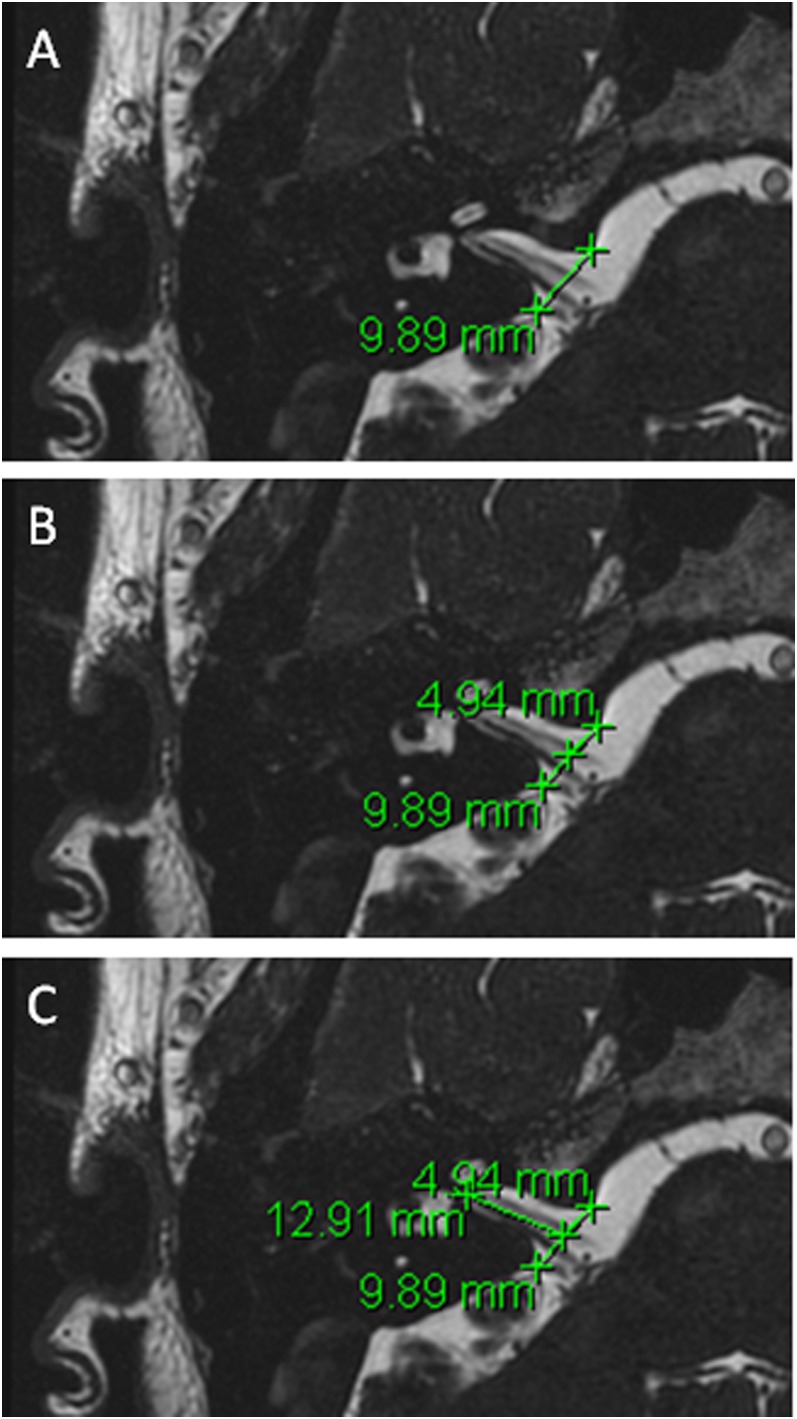
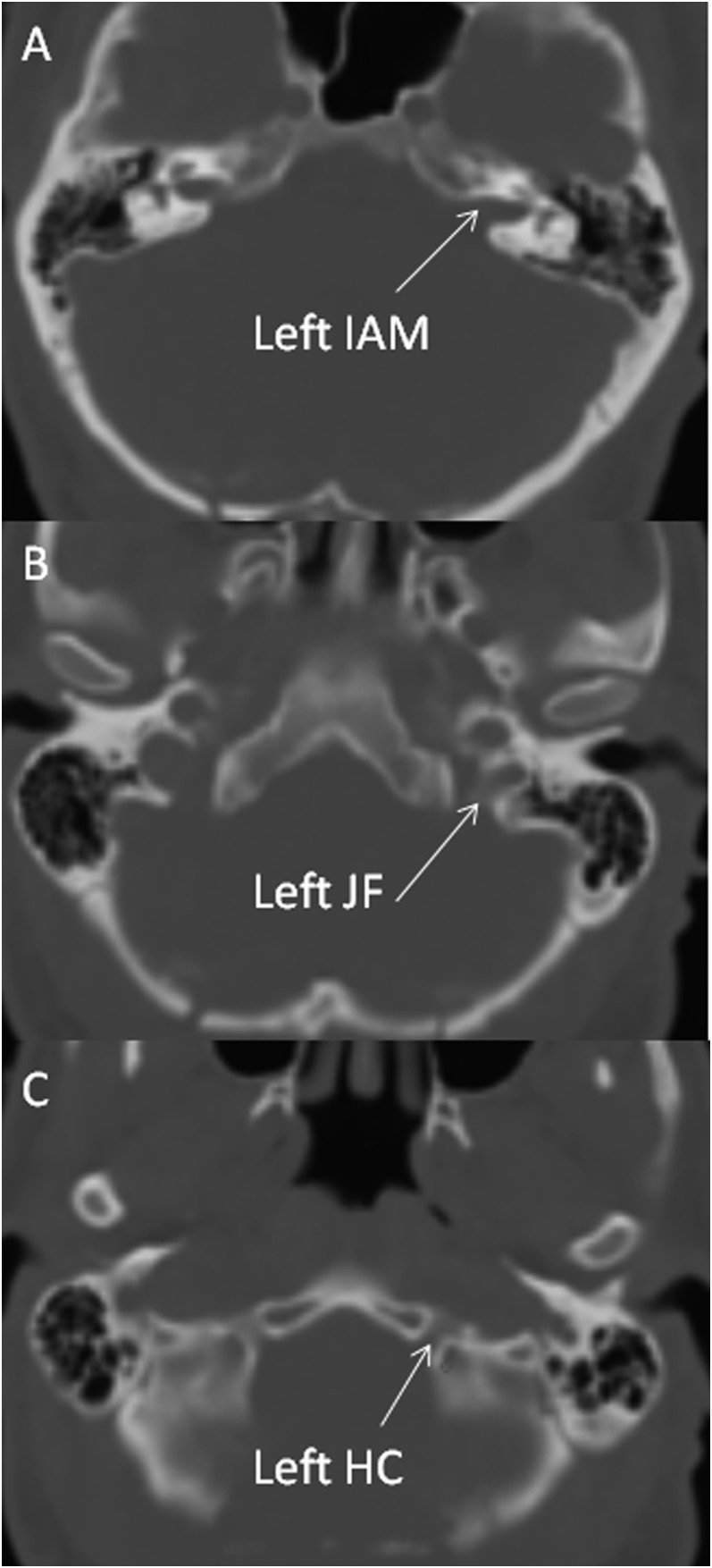
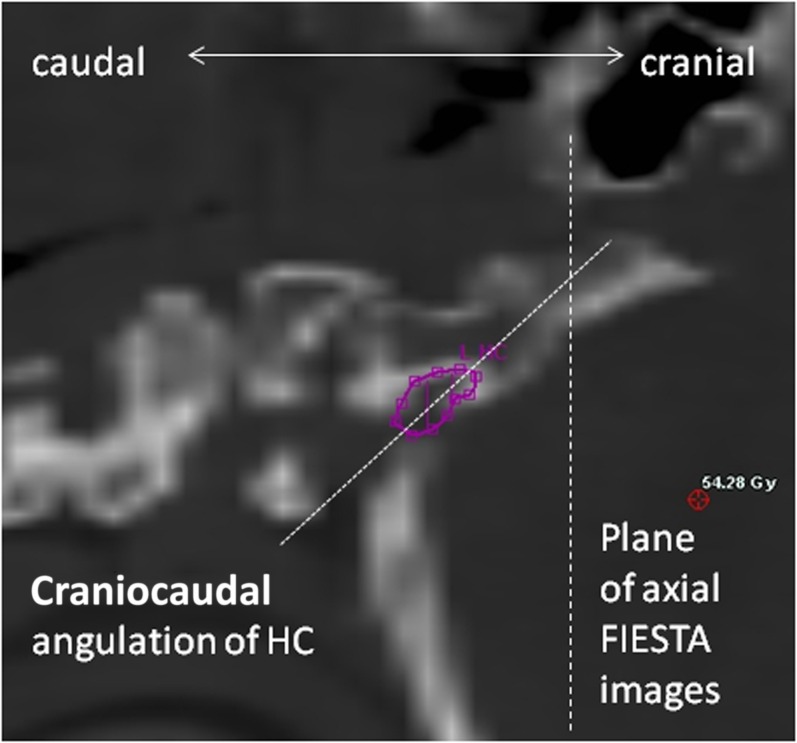
Methods: 96 posterior fossa FIESTA sequences were reviewed. Following exclusions, measurements were made on the following scans for each foramen respectively (left, right); internal acoustic meatus (IAM) (86, 84), jugular foramen (JF) (83, 85) and hypoglossal canal (HC) (42, 45). A protocol describes measurement procedure. Two observers measured distances for five cases and agreement was assessed. One observer measured all the remaining cases.
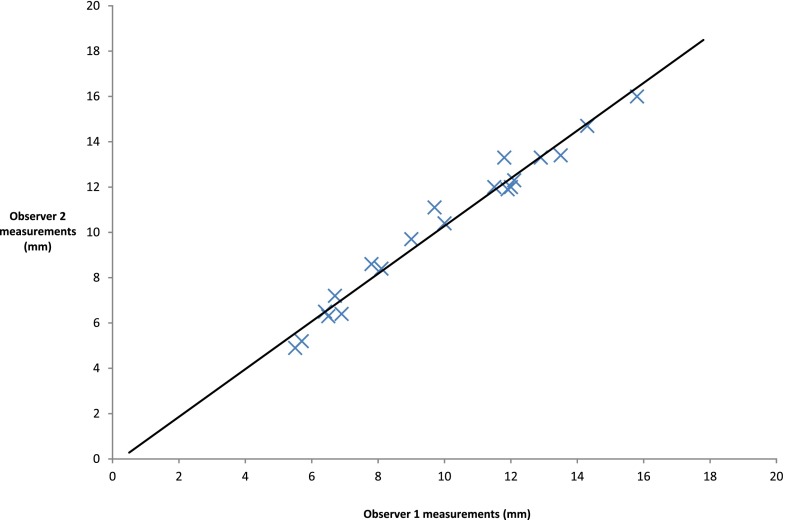
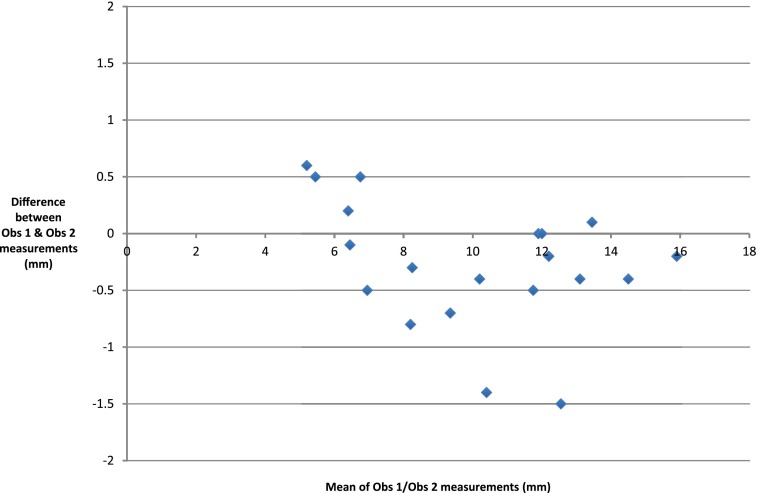
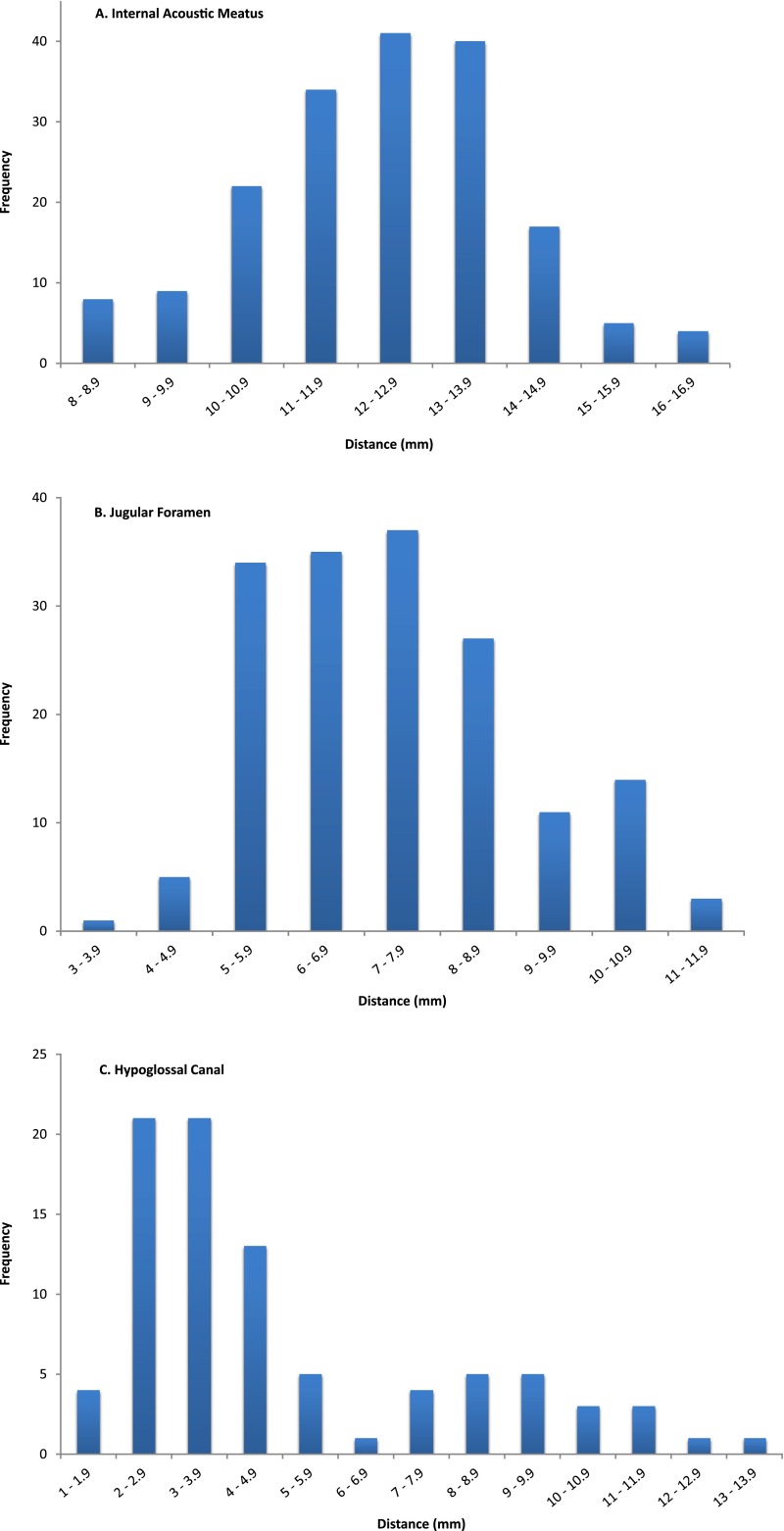
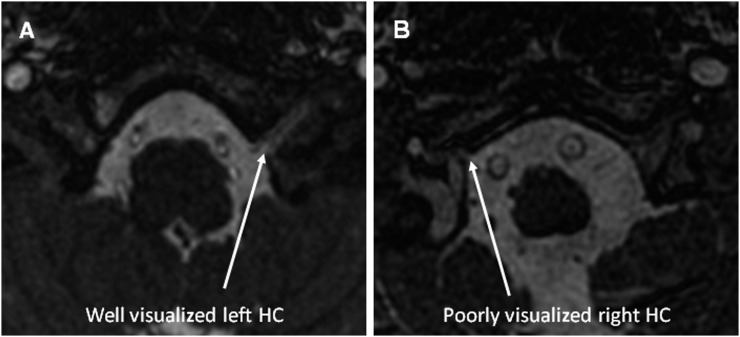
Results: IAM and JF measurement interobserver variability was compared. Mean measurement difference between observers was -0.275 mm (standard deviation 0.557). IAM and JF measurements were normally distributed. Mean IAM distance was 12.2 mm [95% confidence interval (CI) 8.8-15.6]; JF was 7.3 mm (95% CI 4.0-10.6). The HC was difficult to visualize on many images and data followed a bimodal distribution.
Conclusion: Dural reflections of posterior fossa CNs are well demonstrated by FIESTA MRI. Measuring CSF extension into these structures is feasible and robust; mean CSF extension into IAM and JF was measured. We plan further work to assess coverage of these structures with photon and proton RT plans. Advances in knowledge: We have described CSF extension beyond the internal table of the skull into the IAM, JF and HC. Oncologists planning RT for patients with medulloblastoma and ependymoma may use these data to guide contouring.
Figures
References
-
- Carrie C, Alapetite C, Mere P, Aimard L, Pons A, Kolodie H, et al. . Quality control of radiotherapeutic treatment of medulloblastoma in a multicentric study: the contribution of radiotherapy technique to tumour relapse. The French Medulloblastoma Group. Radiother Oncol 1992; 24: 77–81. doi: 10.1016/0167-8140(92)90282-Y - DOI - PubMed
-
- Taylor RE, Bailey CC, Robinson KJ, Weston CL, Ellison D, Ironside J, et al. . Impact of radiotherapy parameters on outcome in the International Society of Paediatric Oncology/United Kingdom Children's Cancer Study Group PNET-3 study of preradiotherapy chemotherapy for M0–M1 medulloblastoma. Int J Radiat Oncol Biol Phys 2004; 58: 1184–93. doi: 10.1016/j.ijrobp.2003.08.010 - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
