

Initial orthostatic hypotension in teenagers and young adults
- PMID: 27637670
- PMCID: PMC5104795
- DOI: 10.1007/s10286-016-0382-6
Initial orthostatic hypotension in teenagers and young adults
Abstract
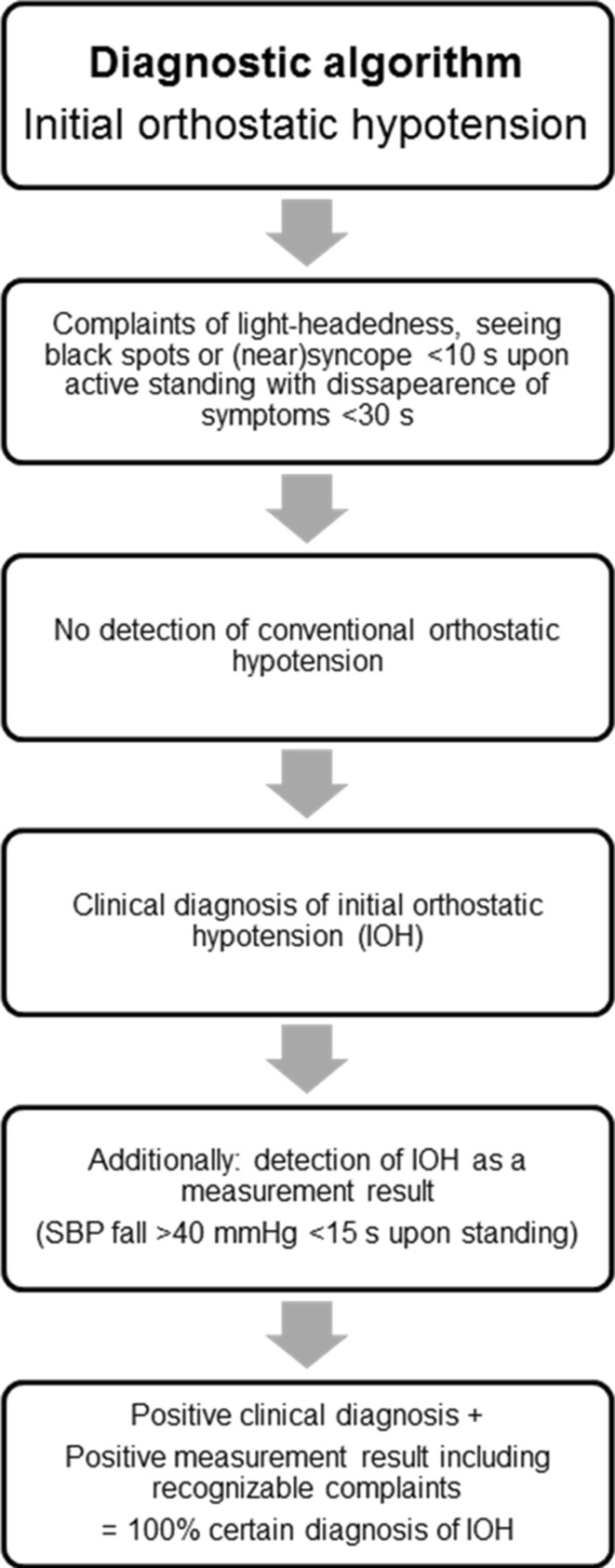
Objective: To assess: (1) the frequency of an abnormally large fall in blood pressure (BP) upon standing from supine in patients with initial orthostatic hypotension (IOH); (2) the underlying hemodynamic mechanisms of this fall in BP upon standing from supine and from squatting.
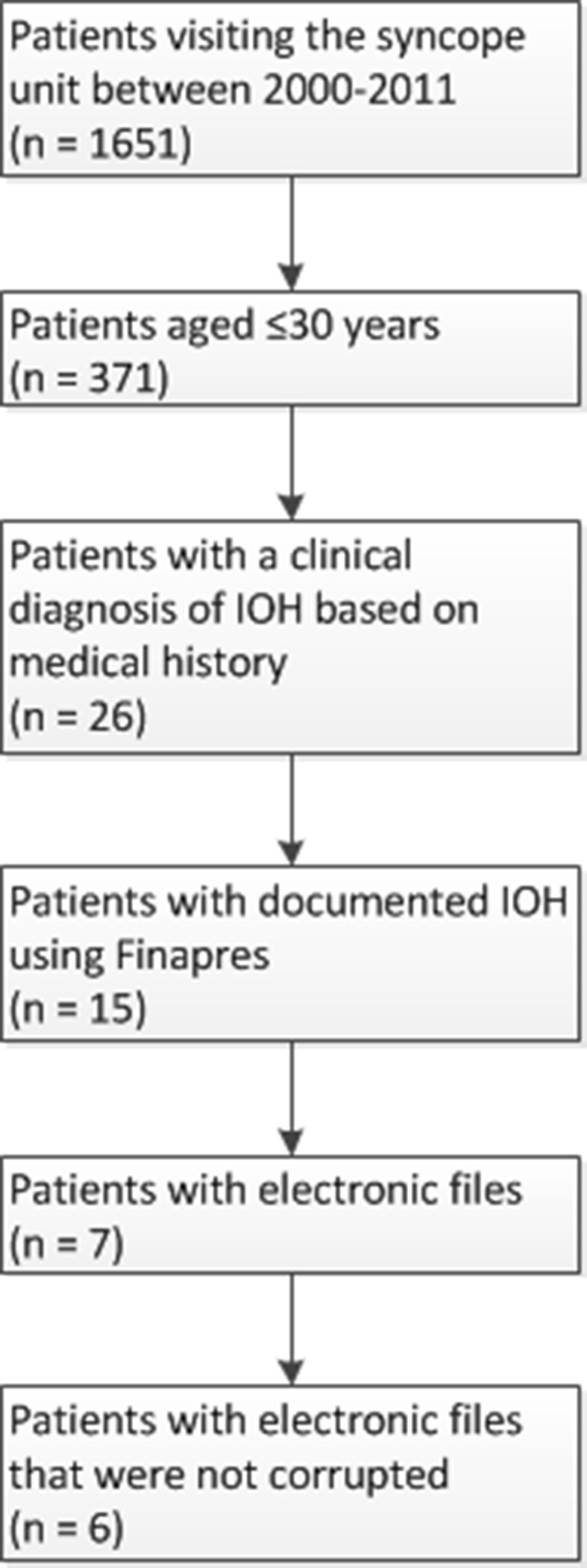
Methods: In a retrospective study of 371 patients (≤30 years) visiting the syncope unit, the hemodynamic response to standing and squatting were studied in 26 patients who were diagnosed clinically with IOH, based on history taking only. In six patients changes in cardiac output (CO) and systemic vascular resistance (SVR) were determined, and the underlying hemodynamics were analyzed.
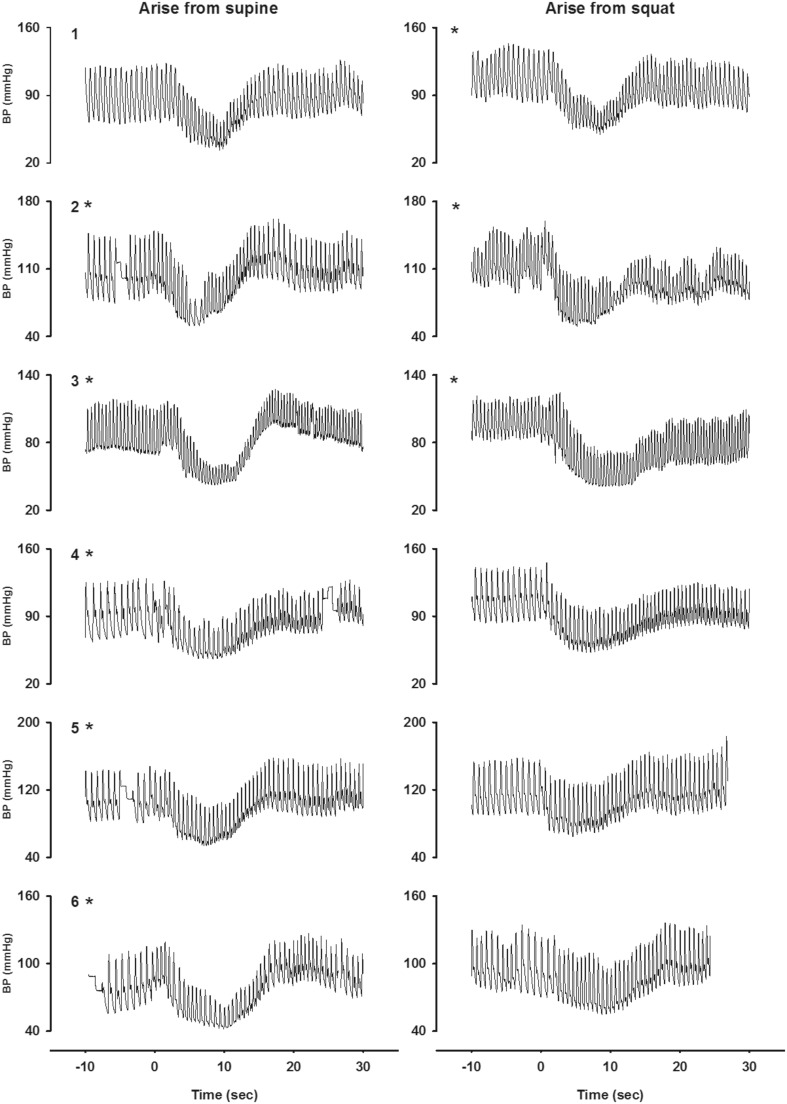
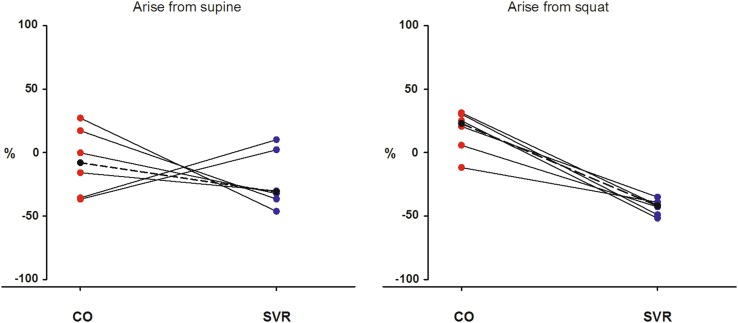
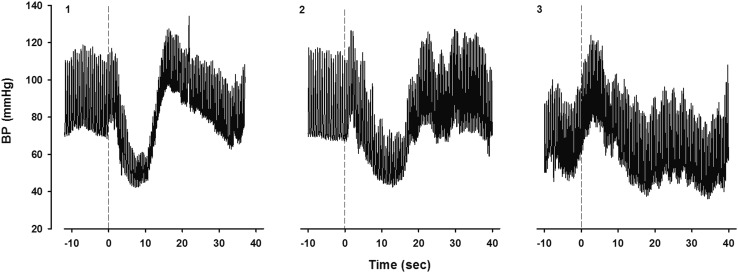
Results: 15/26 (58 %) patients with IOH had an abnormally large initial fall in systolic BP (≥40 mmHg). There was a large scatter in CO and SVR response after arising from supine [ΔCO at BP nadir median -8 % (range -37, +27 %); ΔSVR at BP nadir median -31 % (range -46, +10 %)]. The hemodynamic response after squatting showed a more consistent pattern, with a fall in SVR in all six patients [ΔCO at BP nadir median +23 % (range -12, +31 %); ΔSVR at BP nadir median -42 %, (range -52, -35 %)].
Interpretation: The clinical diagnosis of IOH is based on history taking, as an abnormally large fall in systolic BP can only be documented in 58 %. For IOH upon standing after supine rest, the hemodynamic mechanism can be either a large fall in CO or in SVR. For IOH upon arising from squatting a large fall in SVR is a consistent finding.
Keywords: Blood pressure; Cardiac output; Finapres; Initial orthostatic hypotension; Syncope; Vascular resistance.
Conflict of interest statement
On behalf of all authors, the corresponding author states that there is no conflict of interest.
Figures
References
-
- Task Force for the Diagnosis and Management of Syncope. European Society of Cardiology (ESC) European Heart Rhythm Association (EHRA) Heart Failure Association (HFA), Heart Rhythm Society (HRS) Moya A, et al. Guidelines for the diagnosis and management of syncope (version 2009) Eur Heart J. 2009;30(21):2631–2671. doi: 10.1093/eurheartj/ehp298. - DOI - PMC - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
