

The critical care management of spontaneous intracranial hemorrhage: a contemporary review
- PMID: 27640182
- PMCID: PMC5027096
- DOI: 10.1186/s13054-016-1432-0
The critical care management of spontaneous intracranial hemorrhage: a contemporary review
Abstract
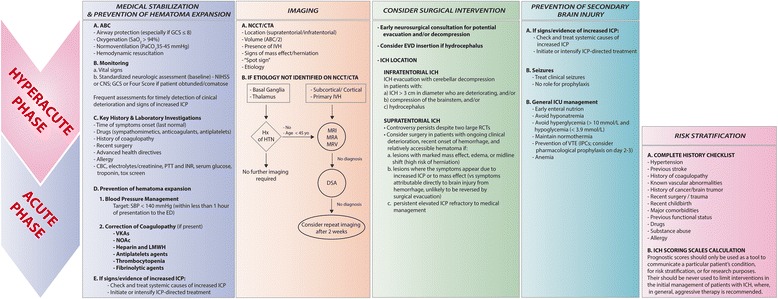
Spontaneous intracerebral hemorrhage (ICH), defined as nontraumatic bleeding into the brain parenchyma, is the second most common subtype of stroke, with 5.3 million cases and over 3 million deaths reported worldwide in 2010. Case fatality is extremely high (reaching approximately 60 % at 1 year post event). Only 20 % of patients who survive are independent within 6 months. Factors such as chronic hypertension, cerebral amyloid angiopathy, and anticoagulation are commonly associated with ICH. Chronic arterial hypertension represents the major risk factor for bleeding. The incidence of hypertension-related ICH is decreasing in some regions due to improvements in the treatment of chronic hypertension. Anticoagulant-related ICH (vitamin K antagonists and the newer oral anticoagulant drugs) represents an increasing cause of ICH, currently accounting for more than 15 % of all cases. Although questions regarding the optimal medical and surgical management of ICH still remain, recent clinical trials examining hemostatic therapy, blood pressure control, and hematoma evacuation have advanced our understanding of ICH management. Timely and aggressive management in the acute phase may mitigate secondary brain injury. The initial management should include: initial medical stabilization; rapid, accurate neuroimaging to establish the diagnosis and elucidate an etiology; standardized neurologic assessment to determine baseline severity; prevention of hematoma expansion (blood pressure management and reversal of coagulopathy); consideration of early surgical intervention; and prevention of secondary brain injury. This review aims to provide a clinical approach for the practicing clinician.
Figures
References
-
- van Asch CJ, Luitse MJ, Rinkel GJ, van der Tweel I, Algra A, Klijn CJ. Incidence, case fatality, and functional outcome of intracerebral haemorrhage over time, according to age, sex, and ethnic origin: a systematic review and meta-analysis. Lancet Neurol. 2010;9(2):167–76. doi: 10.1016/S1474-4422(09)70340-0. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
