

Efficacy and Safety of Metreleptin in Patients with Partial Lipodystrophy: Lessons from an Expanded Access Program
- PMID: 27642538
- PMCID: PMC5026130
- DOI: 10.4172/2155-6156.1000659
Efficacy and Safety of Metreleptin in Patients with Partial Lipodystrophy: Lessons from an Expanded Access Program
Abstract
Objective: Patients with lipodystrophy have severe metabolic abnormalities (insulin resistance, diabetes, and hypertriglyceridemia) that may increase morbidity and mortality. Metreleptin is approved by the United States Food and Drug Administration for treatment of generalized forms of lipodystrophy. We aimed to determine the efficacy and safety of metreleptin among patients with partial lipodystrophy using an expanded-access model.
Methods: Study FHA101 (ClinicalTrials.gov identifier: NCT00677313) was an open-label, expanded-access, long-term clinical effectiveness and safety study in 23 patients with partial lipodystrophy and diabetes and/or hypertriglyceridemia with no prespecified leptin level. Metreleptin was administered subcutaneously at 0.02 mg/kg twice daily (BID) at Week 1, followed by 0.04 mg/kg BID at Week 2. Dose adjustments thereafter were based on patient response (maximum dose of 0.08 mg/kg BID). One-year changes in glycated hemoglobin (HbA1c), fasting plasma glucose, triglycerides, alanine and aspartate aminotransferases, and treatment-emergent adverse events (TEAEs) were evaluated.
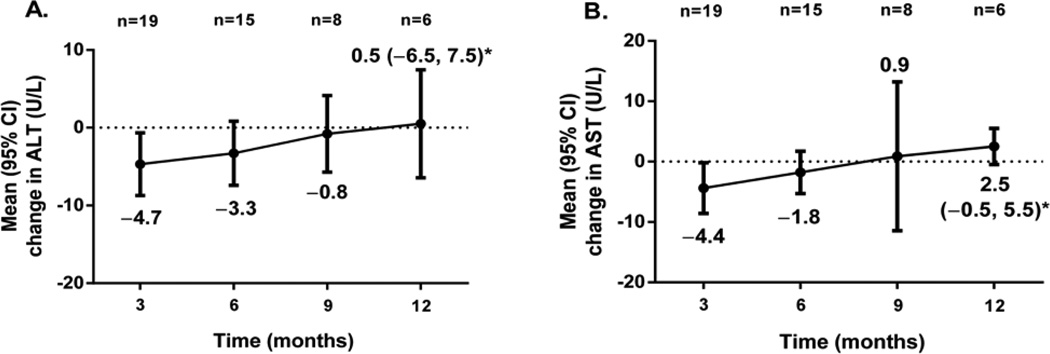
Results: HbA1c, fasting plasma glucose, and triglycerides were numerically decreased throughout 1 year, with mean (standard error) changes from baseline of -0.88 (0.62)%, -42.0 (22.4) mg/dL, and -119.8 (84.1) mg/dL, respectively, which were greater among patients with higher baseline abnormalities. Liver enzymes did not worsen, and the most frequently observed TEAEs (≥ 10% incidence) were mild to moderate and included nausea (39.1%), hypoglycemia (26.1%), and urinary tract infections (26.1%)-all reported previously. There were no reports of clinically significant immune-related adverse events or new safety signals.
Conclusions: Our clinical observations document the large heterogeneity and disease burden of partial lipodystrophy syndromes and suggest that metreleptin treatment benefits may extend to patients with partial lipodystrophy. Additional studies are needed to confirm these preliminary findings.
Keywords: Diabetes; Hypertriglyceridemia; Metreleptin; Partial lipodystrophy.
Figures




References
-
- Chan JL, Oral EA. Clinical classification and treatment of congenital and acquired lipodystrophy. Endocr Pract. 2010;16:310–323. - PubMed
-
- Miehle K, Porrmann J, Mitter D, Stumvoll M, Glaser C, et al. Novel peroxisome proliferator-activated receptor gamma mutation in a family with familial partial lipodystrophy type 3. Clin Endocrinol (Oxf) 2016;84:141–148. - PubMed
-
- Garg A, Peshock RM, Fleckenstein JL. Adipose tissue distribution pattern in patients with familial partial lipodystrophy (Dunnigan variety) J Clin Endocrinol Metab. 1999;84:170–174. - PubMed
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical