

Early Experience of Robotic Hysterectomy for Treatment of Benign Uterine Disease
- PMID: 27643518
- PMCID: PMC10309490
- DOI: 10.1055/s-0036-1592345
Early Experience of Robotic Hysterectomy for Treatment of Benign Uterine Disease
Abstract
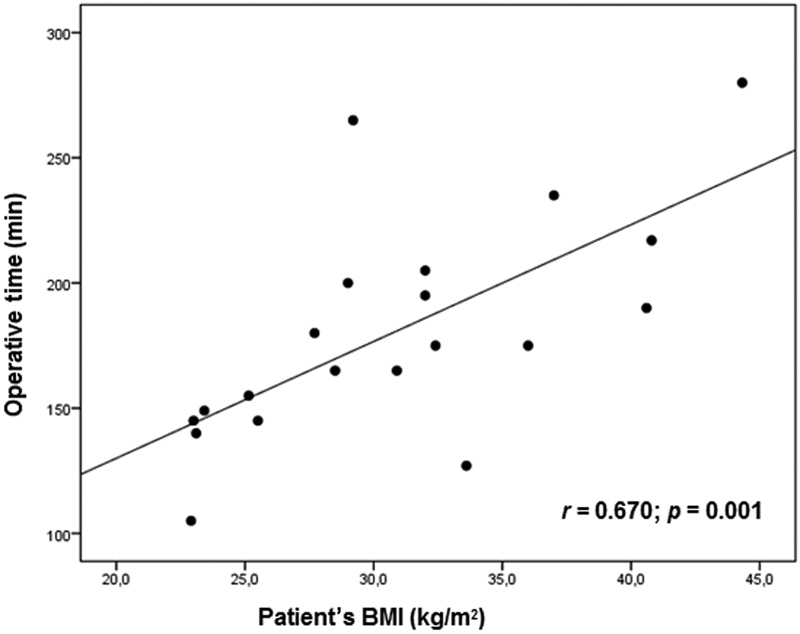
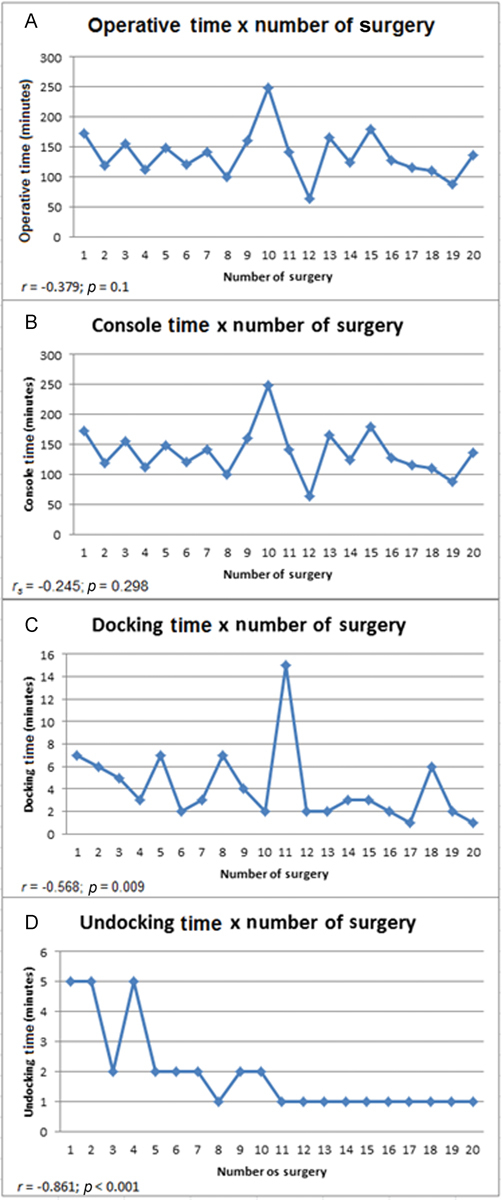
Objectives To demonstrate the initial experience of robotic hysterectomy to treat benign uterine disease at a university hospital in Brazil. Methods A cross-sectional study was conducted to review data from the first twenty patients undergoing robotic hysterectomy at our hospital. The surgeries were performed from November 2013 to August 2014, all of them by the same surgeon. The patients were reviewed for preoperative characteristics, including age, body mass index (BMI), indications for the hysterectomy and previous surgeries. Data of operative times, complications, postoperative pain and length of hospital stay were also collected. Results The total operating room time was 252.9 minutes, while the operative time was 180.7 minutes and the console time was 136.6 minutes. Docking time was 4.2 minutes, and the average undocking time was 1.9 minutes. There was a strong correlation between the operative time and the patient's BMI (r = 0.670; p = 0.001). The console time had significant correlation with the uterine weight and the patient's BMI (r = 0.468; p = 0.037). A learning curve was observed during docking and undocking times. Conclusion Despite its high cost, the robotic surgery is gaining more space in gynecological surgery. By the results obtained in our hospital, this surgical proposal proved to be feasible and safe. Our initial experience demonstrated a learning curve in some ways.
Resumo: Objetivos O presente projeto visa à documentação da experiência inicial do Hospital de Clínicas de Porto Alegre na realização da histerectomia robótica.
Métodos Um estudo transversal foi realizado a fim de revisar dados das primeiras vinte pacientes submetidas à histerectomia robótica em nosso hospital. As cirurgias foram realizadas no período de novembro de 2013 a agosto de 2014, e todas tiveram o mesmo cirurgião. Foram analisadas características pré-operatórias, incluindo idade, índice de massa corporal, cirurgias prévias abdominais, paridade, indicação da histerectomia. Dados referentes aos tempos operatórios, complicações, dor pós-operatória e tempo de internação pós-operatória também foram coletados.
Resultados O tempo de sala total foi de 252,9 minutos, enquanto o tempo cirúrgico total foi 180,7 minutos, e o tempo de console foi 136,6 minutos. O tempo médio de docking foi 4,2 minutos; e o tempo médio de undocking foi 1,9 minutos. Foi observada forte correlação entre o tempo cirúrgico total e o índice de massa corporal da paciente (r = 0,670; p = 0,001). O tempo de console teve correlação significativa com o peso uterino e com o índice de massa corporal das pacientes (r = 0,468; p = 0,037). Foi observada curva de aprendizado nos tempos de docking e undocking.
Conclusão Apesar do alto custo, a robótica vem ganhando espaço na cirurgia ginecológica. Pelos resultados obtidos no nosso hospital, a proposta provou ser factível e segura. Nossa experiência inicial demonstrou curva de aprendizado em alguns aspectos.
Thieme Publicações Ltda Rio de Janeiro, Brazil.
Figures
Similar articles
-
Initial experience with single-port robotic hysterectomy.Einstein (Sao Paulo). 2017 Oct-Dec;15(4):476-480. doi: 10.1590/S1679-45082017AO4134. Einstein (Sao Paulo). 2017. PMID: 29364368 Free PMC article.
-
Gynecologic robotic laparoendoscopic single-site surgery: prospective analysis of feasibility, safety, and technique.Am J Obstet Gynecol. 2015 Feb;212(2):179.e1-8. doi: 10.1016/j.ajog.2014.07.057. Epub 2014 Aug 1. Am J Obstet Gynecol. 2015. PMID: 25088863
-
Feasibility and Learning Curve of Robotic Laparoendoscopic Single-Site Surgery in Gynecology.J Minim Invasive Gynecol. 2017 Feb;24(2):323-328. doi: 10.1016/j.jmig.2016.11.007. Epub 2016 Nov 17. J Minim Invasive Gynecol. 2017. PMID: 27867048
-
[Gynecologic robotic surgery and our initial experience].Ceska Gynekol. 2010 Dec;75(6):512-7. Ceska Gynekol. 2010. PMID: 27534006 Review. Czech.
-
Review of strategies and factors to maximize cost-effectiveness of robotic hysterectomies and myomectomies in benign gynecological disease.J Robot Surg. 2019 Oct;13(5):635-642. doi: 10.1007/s11701-019-00948-9. Epub 2019 Mar 27. J Robot Surg. 2019. PMID: 30919259 Review.
Cited by
-
Safe Implementation of Robotic Surgery for Gynecologic Diseases at a Tertiary Center: Retrospective Analysis of 149 Cases and Review of the Literature.Gynecol Minim Invasive Ther. 2024 Dec 27;14(1):33-39. doi: 10.4103/gmit.gmit_144_23. eCollection 2025 Jan-Mar. Gynecol Minim Invasive Ther. 2024. PMID: 40143989 Free PMC article.
References
-
- Davies A, Hart R, Magos A, Hadad E, Morris R. Hysterectomy: surgical route and complications. Eur J Obstet Gynecol Reprod Biol. 2002;104(2):148–151. - PubMed
-
- Kovac S R, Barhan S, Lister M, Tucker L, Bishop M, Das A. Guidelines for the selection of the route of hysterectomy: application in a resident clinic population. Am J Obstet Gynecol. 2002;187(6):1521–1527. - PubMed
-
- Falcone T, Walters M D. Hysterectomy for benign disease. Obstet Gynecol. 2008;111(3):753–767. - PubMed
-
- Brasil Ministério da Saúde. DATASUS [Internet]. Histerectomias: procedimentos hospitalares do SUS por região de internação 2012 [citado 2015 Nov 10]. Disponível em:http://tabnet.datasus.gov.br/cgi/tabcgi.exe?sih/cnv/qiuf.def
-
- Cruz F O Instituto de Comunicação e Informação Científica e Tecnologia em Saúde [Internet] Histerectomia. 2012 [citado 2015 Dez 12]. Disponível em: http://www.proadess.icict.fiocruz.br/index.php?pag=fic&cod=G01&tab=1
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical